
The “Three-column” concept has significant prognostic value in addition to guiding surgical planning in proximal tibial fractures. Increasing column involvement in such fractures is associated with progressively poorer early functional outcomes and higher complication rates.
Dr. Avik Kumar Naskar, Department of Orthopaedics, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. E-mail: avik7933@gmail.com
Abstract
Introduction: The three-column concept has enhanced understanding of proximal tibial fracture morphology and surgical planning. However, its role as a prognostic indicator remains underexplored. This study evaluates whether column involvement predicts early functional outcome and complications.
Materials and Methods: A prospective study of 30 patients with proximal tibial fractures treated with open reduction and internal fixation was conducted. Fractures were classified into single-, two-, and three-column injuries. Functional outcomes were assessed using the modified Rasmussen score at follow-up of 8 months. Complications were recorded. Statistical analysis was performed using analysis of variance and chi-square tests.
Results: Single-column fractures showed predominantly excellent outcomes, while three-column fractures had a higher proportion of fair to poor outcomes. A statistically significant association was observed between increasing column involvement and poorer functional outcome (P < 0.001). Complications were more frequent in fractures involving multiple columns, especially three-column injuries.
Conclusion: Column involvement is a significant determinant of early outcome in proximal tibial fractures. Increasing fracture complexity predicts poorer functional results and higher complication rates, highlighting the prognostic relevance of the three-column concept.
Keywords: Tibial plateau fracture, three-column concept, functional outcome, prognosis, open reduction and internal fixation.
Proximal tibial fractures are complex intra-articular injuries that require precise anatomical reduction and stable fixation to restore knee function. Conventional classification systems, such as Schatzker classification, although widely used, do not adequately account for posterior column involvement, which has important implications for surgical management [1]. Yang et al. described that posterior tibial fracture is common in high-velocity trauma, and a computed tomography (CT)-based classification is much needed to understand the fracture morphology and mechanism of injuries [2]. The “three-column” concept (Table 1), introduced by Luo et al. in 2010, divides the proximal tibia into medial, lateral, and posterior columns based on CT, thereby improving fracture characterisation and guiding surgical approaches [3].
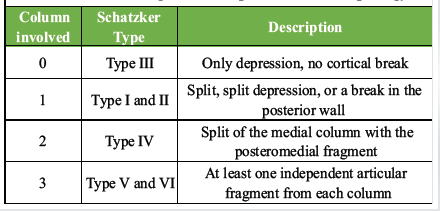
Table 1: Correlation between the number of columns involved in proximal tibial plateau fractures and corresponding Schatzker classification, along with descriptive fracture morphology
This system has the advantage of identifying the posteromedial fracture fragment, which requires buttressing through a posteromedial approach. While the three-column concept (Fig. 1) has been extensively used for surgical planning, its role as a prognostic indicator has not been sufficiently evaluated.
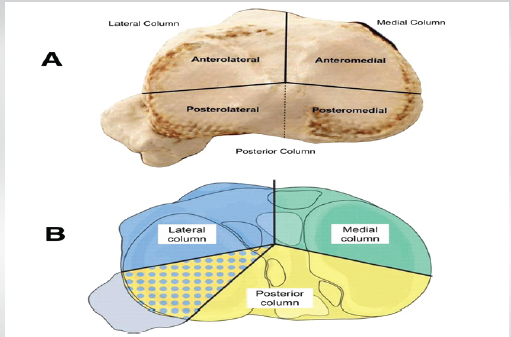
Figure 1: Illustration of the three-column concept of the proximal tibia; (a) Cadaveric axial view of the tibial plateau demonstrating division into anterolateral, anteromedial, posterolateral, and posteromedial regions based on medial, lateral, and posterior columns and, (b) schematic representation highlighting the three-column classification- lateral (blue), medial (green), and posterior (yellow) columns, with the posterolateral fragment (dotted area) emphasizing its distinct morphological and surgical relevance.
This study aims to assess whether the number of columns involved correlates with early functional outcome and complication rates in proximal tibial fractures.
The study was conducted at the Department of Orthopaedics in a tertiary care facility and was approved by the Ethics Committee of the institute (ethics code: IGGMC/Pharm/BORS/1504–05/2023) on July 22, 2023.
Study population:
A total of 30 patients, including 22 males and eight females, undergoing open reduction and internal fixation of proximal tibial fractures between April 2022 and April 2024 were considered eligible and were included in the study.
Study design:
This is a prospective observational study conducted in the Department of Orthopaedics to evaluate and prognosticate proximal tibial fractures treated with open reduction and internal fixation (ORIF) using the “three-column” concept.
Data source:
The study investigated patients who were operated between April 2022 and April 2024. The Ethics Committee of the Institute approved the study.
Inclusion criteria:
- Age ≥15 years
- Closed proximal tibial fractures.
Exclusion criteria:
- Age <15 years
- Open fractures
- Pathological fractures
- Associated neurovascular injury
- Loss to follow-up.
Data collection:
From the surgical operating data, investigations, such as pre- and post-operative imaging and demographic information, including age, gender, body habitus, and prior functional activity, were gathered. A comprehensive clinical examination was done, including the evaluation of the neurovascular status of all the patients before consideration for ORIF. Plain radiographs with a 15° caudal view were taken to visualise the articular surface in doubtful fractures. From the axial CT imaging of the knee joint, the three columns of the tibial plateau were identified and articular depression assessed (Figs. 2, 3, 4).
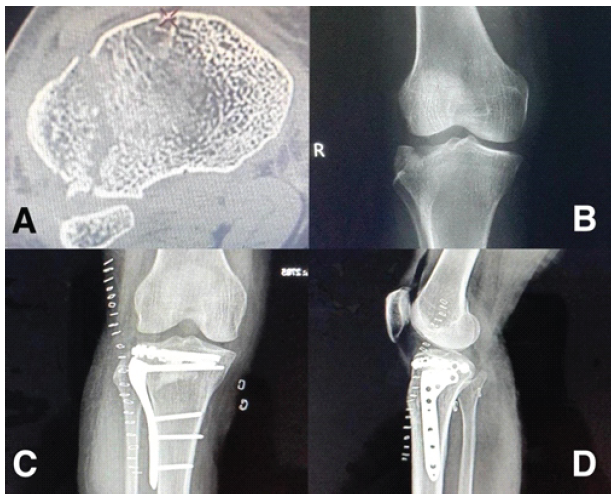
Figure 2: Pre- and post-operative radiological evaluation of a proximal tibial plateau fracture; (a) Axial computed tomography image demonstrating an articular fragment involving the lateral tibial plateau. (b) Pre-operative anteroposterior radiograph of the right knee showing a lateral tibial plateau fracture with articular depression. (c) Immediate post-operative anteroposterior radiograph demonstrating fixation with a proximal tibial locking plate and screws with restoration of joint congruity. (d) Post-operative lateral radiograph confirming adequate reduction, implant positioning, and restoration of the articular surface.
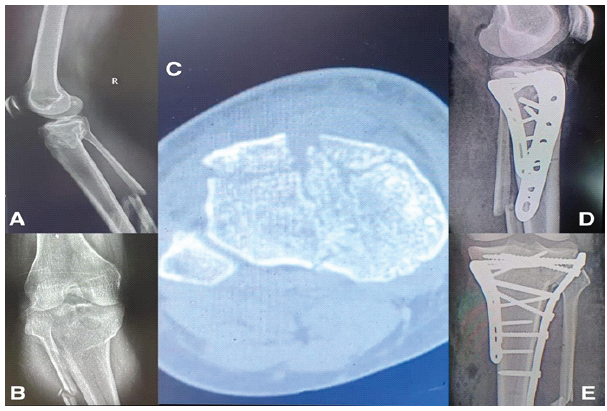
Figure 3: Pre-operative imaging, computed tomographic evaluation, and post-operative fixation of a proximal tibial plateau fracture; (a) pre-operative lateral radiograph of the right knee showing a proximal tibial fracture with metaphyseal extension. (b) Pre-operative anteroposterior radiograph demonstrating involvement of the tibial plateau with articular disruption. (c) Axial computed tomographic image delineating fracture morphology and articular depression, aiding in column-wise assessment and surgical planning. (d) Immediate post-operative lateral radiograph showing fixation with a proximal tibial locking plates and screws with restoration of alignment. (e) Post-operative anteroposterior radiograph confirming stable fixation, appropriate implant positioning, and satisfactory articular reduction.
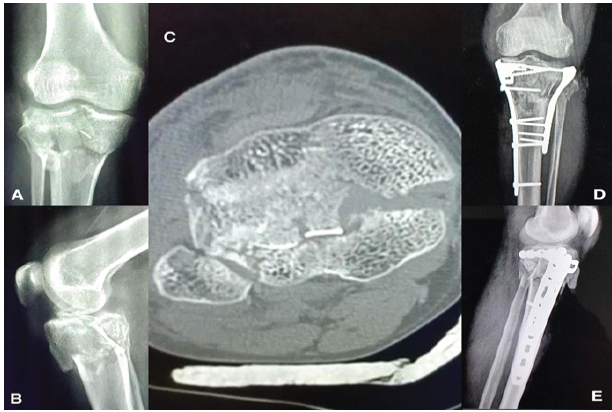
Figure 4: Pre-operative imaging, computed tomographic evaluation, and immediate post-operative radiological images of a proximal tibia fracture; (a) pre-operative anteroposterior and (b) lateral radiographs of the knee showing a complex proximal tibial plateau fracture with articular disruption. (c) Axial computed tomographic scan demonstrating a three-column fracture pattern with involvement of the medial, lateral, and posterior columns. (d) Immediate post-operative anteroposterior and (e) lateral radiographs showing anatomical reduction and stable fixation using locking plates and screws.
Fractures were classified into single-, two-, and three-column injuries based on CT evaluation (Table 2). All patients underwent ORIF using appropriate implants depending on fracture configuration. Early functional outcome was assessed using the Modified Rasmussen score at a follow-up of 8 months [4].
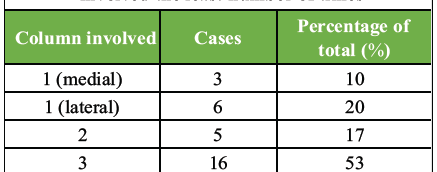
Table 2: Distribution of proximal tibia fracture cases according to column involvement; Majority fractures in the cohort had a three-column involvement, with the isolated medial column being involved the least number of times
Surgical technique:
For fractures involving the lateral and posteromedial columns, a floating position (also referred to as a floppy lateral position) was used because of the advantage of performing both the posteromedial approach (by internal rotation of the leg) and the anterolateral approach (by external rotation) [5]. Other single-column fractures were treated with standard approaches. Synthetic bone graft substitutes or grafts from the ipsilateral iliac crest were used in depressed and comminuted fractures.
Rehabilitation and follow-up protocol:
Post-operatively, the patients were given an above-knee Plaster of Paris slab for immobilisation or compression bandage for 1 week. Passive range of motion (ROM) of the knee joint was started from the 2nd week. The sutures were removed on the 15th day. The patients were encouraged to do static quadriceps exercises for the initial 2 weeks, followed by passive knee ROM and non-weight-bearing crutch-walking, taking the support of the unaffected limb up to 6 weeks. After that, assisted weight-bearing crutch-walking was started. Clinico-radiological follow-ups were done at 6 weeks; 3, 6 (Figs. 5, 6, 7) and 8 months.
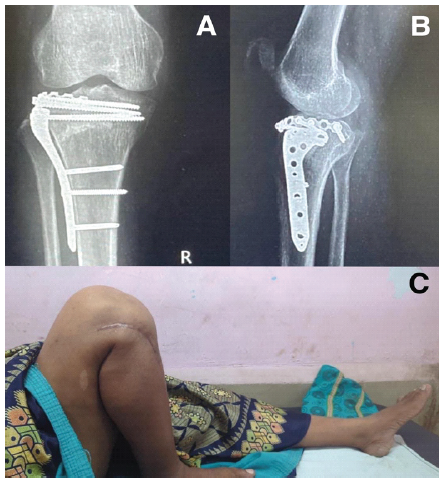
Figure 5: Six-month post-operative radiological and clinical outcome following fixation of a right-sided proximal tibial plateau fracture; (a) Anteroposterior radiograph at 6 months demonstrating maintained reduction, satisfactory alignment, and stable implant in situ with evidence of fracture union. (b) Lateral radiograph at 6 months confirming preservation of articular congruity and appropriate implant positioning. (c) Clinical photograph showing a well-healed surgical scar with full knee range of motion and satisfactory functional outcome.

Figure 6: Six-month post-operative radiological and clinical outcome following fixation of a right-sided proximal tibia fracture; (a) anteroposterior radiograph showing maintained reduction, and stable implant in situ with evidence of fracture union. (b) Lateral radiograph confirming the articular congruity. Clinical images demonstrating a (c) healed surgical scar with normal flexion and (d) Extension of the right knee at 6 months.

Figure 7: Six-month post-operative radiological and clinical outcome following fixation of a proximal tibia fracture; 6-month post-operative (a) anteroposterior and (b) lateral radiographs of the right knee showing maintained reduction and stable bicolumnar plate fixation of the proximal tibial plateau fracture with signs of fracture union. (c and d) Clinical photographs at 6 months demonstrating restricted knee range of motion, with limited flexion and incomplete extension.
Based on the signs of union, gradual progression to full weight-bearing was encouraged. Functional evaluation was done using the Modified Rasmussen clinical criteria (Table 3).
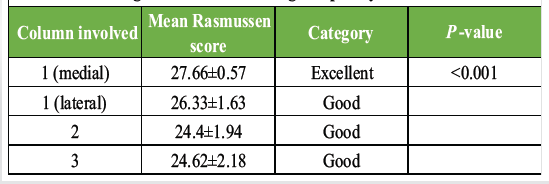
Table 3: Correlation between column involvement and mean clinical Rasmussen score. At post-operative follow-ups, functional outcomes of the knee were assessed using this score, which is based on pain, walking capacity, range of motion, stability, and extension lag. The score showed a decreasing trend with increasing complexity of the fractures
Statistical analysis:
Statistical analysis was performed using analysis of variance and chi-square tests, with significance set at P < 0.05. Continuous variables were expressed as mean ± standard deviation. Changes in functional scores over time were assessed; however, no comparative statistical inference was intended due to the observational nature of the study.
A total of 22 males and eight females with mean ages of 41.68 ± 7.84 years and 51.75 ± 8.33 years, respectively, were included in the study. Road-traffic accidents were the most common indication for surgery, constituting 87% of all cases. The mean age of the 15 patients with right-side involvement was 45.60 ± 8.49 years, and that of the 15 patients with left-side involvement was 43.13 ± 9.70 years.
Functional outcome:
13.33% of the patients had excellent clinical Rasmussen scores, with 70% having good and 16.66% having fair scores. Although surgical site infection was seen in two cases, none had an overall poor score. The highest scores were observed in fractures with only medial column involvement, and the lowest values were seen in three-column involvements.
Complications:
A total of five complications, including two cases of wound infection, knee stiffness each, and one case of screw pull-out, were observed. Out of the two infected patients, one was successfully managed conservatively, and the other required an implant removal. Removal of the pulled-out screw was also done in the corresponding patient. In the two patients who had restricted knee movements, passive ROM exercises were delayed in the immediate postoperative period due to inadequate fixation with articular incongruity in the coronal plane, which ultimately resulted in non-compliance with physiotherapy. Complications were more frequent with increasing column involvement (Table 4). Three-column fractures showed the highest complication rates, including stiffness, infection, and implant-related issues. No statistically significant association was found between age and complications (P > 0.05).
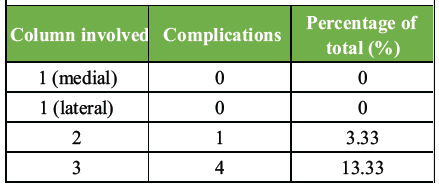
Table 4: Correlation between column involvement and complications observed; Majority complications were seen in proximal tibial fractures with three-column involvement
The majority of displaced and unstable fractures require ORIF, as closed reduction techniques have little success in reducing depressed or displaced fracture fragments. To regain full ROM, stable fracture fixation and ligament repair are critical. While direct visualisation of the fracture, adequate reduction, and stable fixation are advantages of ORIF, there remains an increased risk of soft tissue-related complications, joint stiffness, and infection in the deeper compartments. The present study demonstrates a significant association between increasing column involvement and poorer functional outcomes, along with higher complication rates in proximal tibial fractures. While the three-column concept is well established for fracture characterisation, its prognostic significance has not been adequately emphasised in existing literature. Because of its simplicity, the inter-observer reliability is hugely improved. Luo et al. originally proposed the three-column classification to improve surgical planning and fixation strategies, particularly highlighting the importance of posterior column visualisation using CT imaging [3]. Subsequent studies have underscored the need for addressing posterior fragments to achieve stable fixation and prevent collapse [6]. However, most available literature focuses on surgical techniques rather than outcome prediction. The present study adds to existing knowledge by demonstrating that increasing fracture complexity, as indicated by column involvement, is associated with progressively worse functional outcomes. This suggests that column number can serve as a simple yet effective surrogate marker of injury severity. The higher complication rates observed in three-column fractures may be attributed to multiple factors, including increased comminution, soft tissue compromise, and the technical challenges associated with achieving stable fixation across multiple columns. Similar findings have been reported in studies evaluating high-energy bicondylar fractures, where increased fracture severity correlates with poorer outcomes and higher complication rates [7]. In this study, each case was individualised and treated accordingly. Similarly, the choice of implant was decided based on the fracture pattern, bone quality, and intraoperative reduction achieved. An important finding in this study is that age did not significantly influence complication rates, indicating that fracture morphology may play a more critical role than patient-related factors in determining outcomes. The results achieved in the present study (70% good, 13% excellent, and no poor outcome) are in line with other documented standard studies in the literature [2,8,9]. It is important to note that most other previous studies have reported the outcomes at mid- to long-term follow-up (1–7 years) without shedding light on the prospect of early prognosis [1,3,8,9,10]. The present study with its comparable results provides insight into early recovery following surgery. Unlike previous studies that primarily emphasise the “three-column” concept for surgical planning, the present study, to the best of our knowledge, uniquely evaluates its role as a prognostic tool, thereby addressing a critical gap in the literature regarding early outcome prediction in proximal tibia fractures. From a clinical perspective, this concept should not be limited to pre-operative planning only but also utilised for early prognostication. Surgeons can use column involvement to better counsel patients regarding expected early functional outcomes and potential complication risks.
Limitations of the study:
This study has certain limitations. The relatively small sample size and single-centre design may limit the generalisability of the findings. The short duration of follow-up restricts assessment of long-term functional outcomes, including post-traumatic osteoarthritis and implant-related complications. Future studies with larger cohorts, longer follow-up, and comparative or multivariate analyses are warranted to further validate the prognostic utility of the three-column concept.
Column involvement is a significant determinant of early functional outcome and complication rates in proximal tibial fractures. Increasing fracture complexity, as reflected by the number of columns involved, is associated with progressively poorer outcomes. The three-column concept, therefore, serves not only as a tool for surgical planning but also as a simple and reliable prognostic indicator in clinical practice.
Increasing column involvement predicts poorer early functional outcomes and higher complication rates. The three-column concept helps stratify fracture severity and should be used for both surgical decision-making and early outcome prediction.
References
- 1. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The toronto experience 1968–1975. Clin Orthop Relat Res 1979;138:94-104. [Google Scholar] [PubMed]
- 2. Yang G, Zhai Q, Zhu Y, Sun H, Putnis S, Luo C. The incidence of posterior tibial plateau fracture: An investigation of 525 fractures by using a CT-based classification system. Arch Orthop Trauma Surg 2013;133:929-34. [Google Scholar] [PubMed]
- 3. Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010;24:683-92. [Google Scholar] [PubMed]
- 4. Rasmussen PS. Tibial condylar fractures. Impairment of knee joint stability as an indication for surgical treatment. J Bone Joint Surg Am 1973;55:1331-50. [Google Scholar] [PubMed]
- 5. Lees D, Rankin KS, Marriott A, Murty AN. Floppy lateral position: Technique tip. Foot Ankle Int 2013;34:1460-3. [Google Scholar] [PubMed]
- 6. Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am 2006;88:1713-21. [Google Scholar] [PubMed]
- 7. Egol KA, Tejwani NC, Capla EL, Wolinsky PL, Koval KJ. Staged management of high-energy proximal tibia fractures (OTA types 41): The results of a prospective, standardized protocol. J Orthop Trauma 2005;19:448-55. [Google Scholar] [PubMed]
- 8. Oh CW, Park BC, Kyung HS, Kim SJ, Kim HS, Lee SM, et al. Percutaneous plating for unstable tibial fractures. J Orthop Sci 2003;8:166-9. [Google Scholar] [PubMed]
- 9. Honkonen SE. Indications for surgical treatment of tibial condyle fractures. Clin Orthop Relat Res 1994;302:199-205. [Google Scholar] [PubMed]
- 10. Lansinger O, Bergman B, Körner L, Andersson GB. Tibial condylar fractures. A twenty-year follow-up. J Bone Joint Surg Am 1986;68:13-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery
July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study
May 1, 2026 Functional Outcomes and Surgical Utility of the Modified Schatzker Four-column Concept in Proximal Tibial Plateau Fractures: A Prospective Observational Study October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study
October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study August 1, 2026 Treatment of Bilateral Tibial Tuberosity Avulsion Fractures in a Young Child: A Surgical Case Report
August 1, 2026 Treatment of Bilateral Tibial Tuberosity Avulsion Fractures in a Young Child: A Surgical Case Report