
A well-healed clavicle fracture does not exclude a delayed subclavian artery injury, and unexplained supraclavicular masses warrant further evaluation and vascular imaging in patients with prior clavicle fractures
Miss. Madeline Wethington, University of Minnesota Medical School, 2512 South 7th Street, Minneapolis - 55454, Minnesota, United States. E-mail: wethi008@umn.edu
Abstract
Introduction: The clavicle is one of the most commonly fractured bones and may benefit from operative fixation to restore alignment and function. Although rare, vascular complications are a known risk due to the clavicle’s anatomical proximity to the subclavian vessels. A delayed subclavian artery pseudoaneurysm is a very uncommon but potentially life-threatening complication that surgeons must be aware of, as recognition may be challenging.
Case Report: A 17-year-old female sustained a displaced midshaft clavicle fracture while playing ice hockey and was treated with an open reduction and internal fixation. The fracture healed uneventfully, and the patient returned to full athletic activity. However, nearly 7 years later, the patient presented back with a painless right supraclavicular mass that was initially suspected to be lymphadenopathy caused by Hodgkin’s lymphoma. During the subsequent open biopsy, brisk arterial bleeding revealed a pseudoaneurysm of the right subclavian artery. The lesion was repaired intraoperatively, and the patient recovered without neurological deficit or further vascular complications. Follow-up vascular imaging demonstrated a thrombosed pseudoaneurysm without evidence of ongoing arterial flow; therefore, no further intervention was sought.
Conclusion: A delayed subclavian artery pseudoaneurysm can present several years after a clavicle fracture fixation, even in the absence of radiographic risk factors. Persistent or growing supraclavicular masses, vascular concerns, or exertional neurological symptoms in patients with prior clavicle injury should prompt vascular evaluation.
Keywords: Clavicle fracture, subclavian artery, pseudoaneurysm, vascular complication, orthopedic fixation.
Clavicle fractures are common injuries, typically resulting from falls, sports activities, or motor vehicle accidents, and account for up to 4% of all adult fractures [1,2]. Approximately 80% of these fractures occur at the midshaft because it is the thinnest segment and does not have any ligamentous attachments [1,2]. Their proximity to major neurovascular structures—particularly the subclavian vessels and brachial plexus—poses a serious risk of complications [3]. Neurovascular injuries may arise both from the initial trauma and from surgical intervention. Reported complications include brachial plexopathy, pseudoaneurysm, arteriovenous fistula, deep vein thrombosis, and thoracic outlet syndrome [4]. Subclavian vessel injury is more likely in spiral or oblique fractures, where sharp bone fragments can lacerate adjacent soft tissues [5]. Such injuries can result in haematoma formation, pseudoaneurysm, compromised limb perfusion, or major bleeding requiring urgent surgical repair [5]. While most midshaft clavicle fractures heal successfully with non-operative management, surgical fixation is often indicated for acute fractures with complete displacement, more than 2 cm of shortening, significant comminution, or a Z-type pattern to minimise the risk of symptomatic malunion or non-union and restore clavicular length, alignment, and rotation [6]. This is important because even modest shortening has been linked to worse quick-disabilities of the arm, shoulder, and hand scores and decreased shoulder performance, with shortening as little as 1.3 cm correlating with inferior functional outcomes between operative and non-operative groups [7]. Although the overall incidence of subclavian vessel injury is low, these injuries may be subtle and easily overlooked, particularly in closed or minimally displaced fractures, underscoring the need for a high index of suspicion and careful clinical evaluation [6,8]. We present a rare case of a delayed subclavian artery pseudoaneurysm in a patient following clavicle open reduction and internal fixation (ORIF) with an anterior plate and screws, highlighting the importance of vigilance for delayed vascular complications following clavicular fracture repair.
A 17-year-old right-hand dominant female presented with a closed right mid-shaft clavicular fracture that occurred in an ice-hockey game from direct impact of the hockey puck against the clavicle and a subsequent fall later in the game with her right arm extended across her body. The patient, on physical exam, was neurovascularly intact. Due to the clavicle exhibiting shortening and displacement of >2 cm on X-ray (Fig. 1) as well as her age, high activity level, and right handedness, the patient was indicated for ORIF.
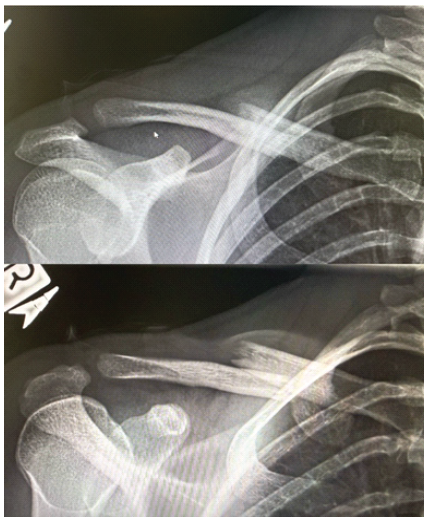
Figure 1: Initial patient X-ray upon right clavicle injury.
Approximately 48 h after injury, the patient underwent ORIF with an anterior placed plate and 8 screws. The patient recovered well with no complications. Post-operative X-rays 8 weeks after surgery displayed a well-healed clavicle (Fig. 2).

Figure 2: Well-healed 8-week post-operative right clavicle X-ray.
The patient returned to playing hockey with full contact and no restrictions. While there were no signs of hardware failure and the patient denied pain, the patient did report numbness at the surgical site.
In the years following surgery, the patient’s only notable symptoms were numbness of the right clavicular area and intermittent discomfort and paresthesia of the right upper extremity that occurred with weight lifting – in particular, bench press, push-ups, and pull-ups. The patient was seen by her orthopedic physician 3 years later regarding these intermittent symptoms and diagnosed with a potential strain of muscles around the plate. However, the chronic intermittence of the symptoms and their reproducibility with upper extremity loading raised concern that a simple muscular strain might not fully explain the patient’s presentation.
Approximately 7 years after clavicular ORIF, the patient presented to her primary care physician due to a palpable mass in her supraclavicular fossa (Fig. 3).
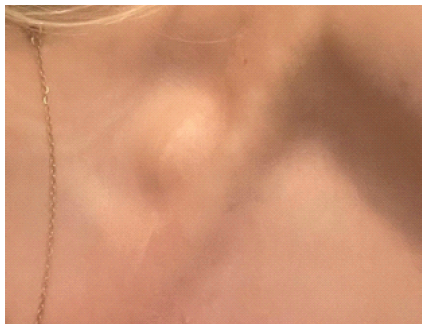
Figure 3: Palpable mass of right supraclavicular fossa underlying skin incision from prior clavicular open reduction and internal fixation.
The differential diagnosis made by the primary care physician included cyst, enlarged lymph node, or lipoma. Subsequent laboratory tests and an ultrasound showed an atypical heterogeneous lymph node with internal calcifications, no definitive fatty hilum, and an adjacent vessel (Fig. 4). An ultrasound-guided percutaneous biopsy or open biopsy due to the adjacent vessel was recommended.
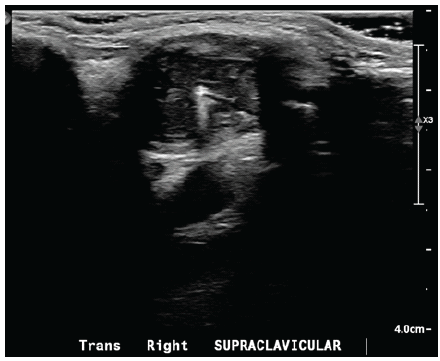
Figure 4: Ultrasound soft tissue head/neck. Limited sonographic evaluation of the supraclavicular on the right at the palpable area of concern demonstrates a heterogeneous 2.1 × 1.8 × 1.4 cm nodule with internal 2 mm calcification. No definitive fatty hilum is identified. There is an adjacent vessel. The remaining surrounding soft tissues are unremarkable. Favor atypical lymph node.
After consultation with a general surgeon, the differential diagnosis included Hodgkin’s lymphoma, and an open biopsy was advised. Approximately 1 month after the ultrasound, the patient was evaluated by a general surgeon for open biopsy of a right supraclavicular mass, which was initially suspected to represent atypical lymphadenopathy concerning for Hodgkin’s lymphoma. An open biopsy of the right supraclavicular subfascial mass was performed. Intraoperatively, the mass was circumferentially dissected and found to be densely adherent to the subclavian vein without a clear plane of separation. Needle aspiration revealed no blood, and a wedge biopsy was performed and sent for histology. Upon resection, brisk arterial bleeding occurred, revealing a connection to the right subclavian artery and prompting concern for a chronic pseudoaneurysm related to the patient’s prior clavicular fracture. Hemostasis was achieved with direct pressure, airway control via intubation, primary repair of the pseudoaneurysm using interrupted 4-0 Prolene sutures, and reinforcement with thrombin-based hemostatic sealant. Estimated blood loss was 50 mL. The final post-operative diagnosis was a right subclavian artery pseudoaneurysm.
Post-operatively, the patient followed up with orthopedic surgery, and an X-ray of the right clavicle showed normal bony morphology, no implant loosening, and adequate screw length and trajectory away from the subclavian vessels, indicating a low likelihood that a screw could be impinging or perforating on the subclavian (Fig. 5). There was also no non-union or malunion seen. The surgeon believed that the mass was not musculoskeletal and did not have to do with malposition of the hardware.
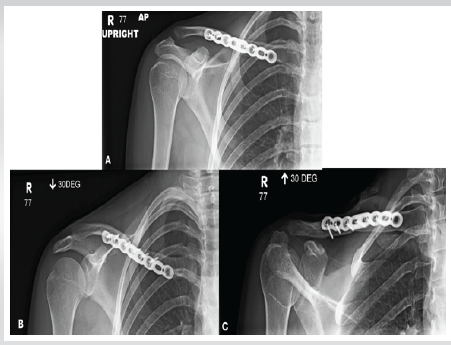
Figure 5: X-ray clavicle right. Surgical fixation of the right clavicle. No unexpected radiopaque foreign body or acute osseous abnormalities.
The patient also had a magnetic resonance angiography and magnetic resonance imaging (MRI) ordered by vascular surgery. The report noted that orthopedic hardware in the right clavicle was causing an artifact and limiting evaluation of surrounding structures. Adjacent small aneurysms were difficult to exclude. Small arteries adjacent to the clavicle could not be evaluated due to susceptibility artifacts from the orthopedic hardware. Deep to the right mid clavicle, there was a mass-like region of isointense T1 and heterogeneous hyperintense T2 signal with mild enhancement and a small central focus of hypointense T1 and hypointense T2 signal that measured approximately 3.2 × 1.5 cm on the axial plane. This lesion was superior to the right subclavian vessels. There did not appear to be osseous involvement. Mass-like lesion deep to the right mid clavicle with heterogeneous T2 signal and mild enhancement is indeterminate, although it could represent fibrosis/scarring or possibly a thrombosed vessel with surrounding inflammatory changes. An aneurysm in this region could not be completely excluded.
Due to the susceptibility artifact on MRI, a computed tomography angiography was ordered, but the right supraclavicular region is obscured by artifact from ORIF hardware. Thus, an ultrasound with Doppler was ordered to examine the right supraclavicular region (Fig. 6).
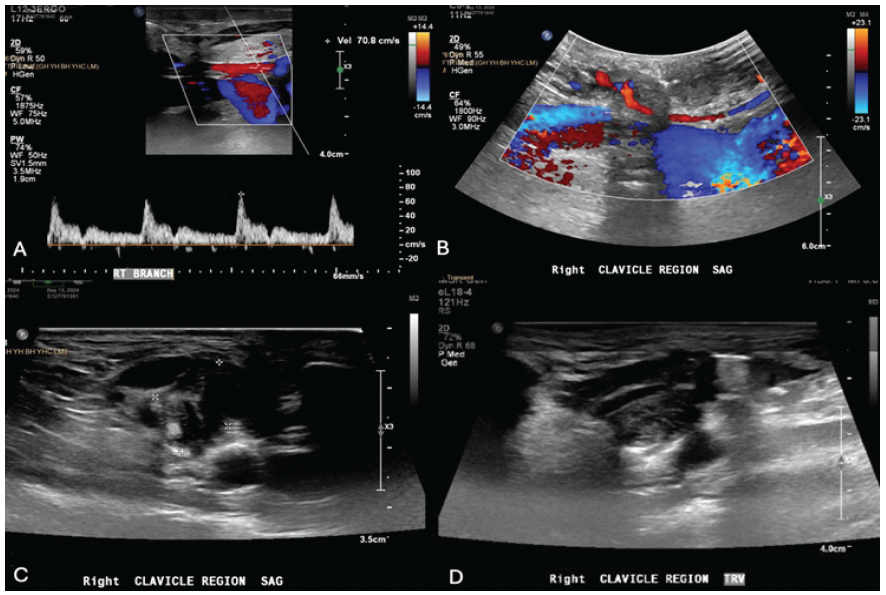
Figure 6: Ultrasound head neck soft tissue. In the right supraclavicular region, there is an approximately 3.3 × 1.5 cm hypoechoic structure that is intimately associated with a small artery and superior to the subclavian vessels, potentially the suprascapular artery or dorsal scapular artery. There is no flow on color Doppler within the hypoechoic structure outside of the artery. The subclavian vessels and cells are unremarkable, with normal venous waveforms in the subclavian vein with no evidence of fistulization to the vessel. This could represent a thrombosed post-operative/post-traumatic pseudoaneurysm or other post-operative/post-traumatic vascular lesion, although there is no flow seen outside of the small artery. This could also represent a soft tissue mass or scar tissue.
Radiologist report noted that a 3.3 × 1.5 cm hypoechoic structure encircling a small artery in the right supraclavicular region likely representing either a thrombosed post-operative/post-traumatic pseudoaneurysm or other post-operative/post-traumatic vascular lesion. Vascular surgery recommended no further treatment or follow-up needed as the chronic pseudoaneurysm appeared thrombosed at this time with no significant blood flow.
The purpose of this case report is not only to describe a rare delayed vascular complication following clavicle fracture fixation, but also to raise awareness of this potentially life-threatening condition. It is crucial for physicians to remain vigilant and attentive to patients’ prior surgical history, particularly clavicle fractures, given the potential for subclavian artery pseudoaneurysm to present years after apparent fracture healing. A review of the literature identified 18 reported cases of pseudoaneurysm formation following clavicle fracture, with or without surgical fixation (Table 1).
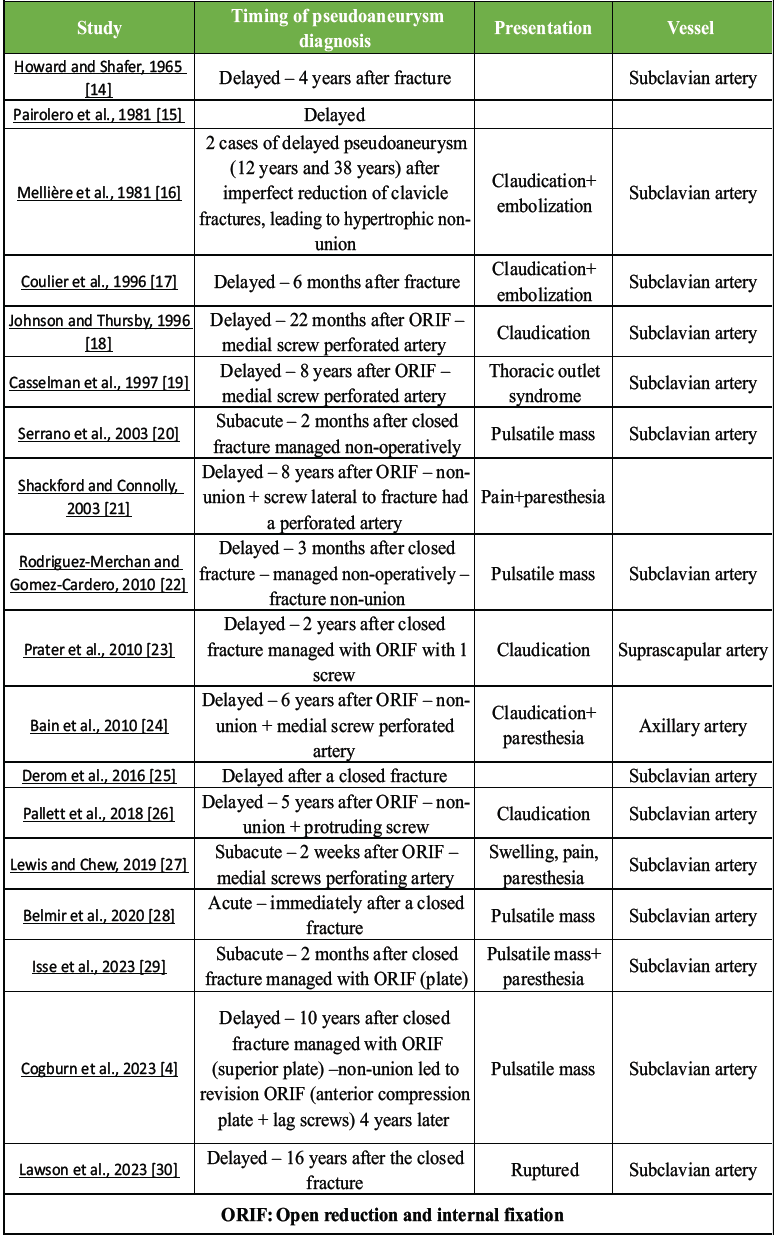
Table 1: Review of the literature found 18 reported cases of pseudoaneurysm formation following clavicle fracture, with or without surgical fixation
Nearly all involved the subclavian artery, with isolated reports involving the suprascapular and axillary arteries. Most cases presented in a delayed or subacute fashion with symptoms, such as a pulsatile mass, pain, swelling, paraesthesia, thoracic outlet syndrome, or distal claudication secondary to peripheral embolisation. Many were associated with fracture non-union or malunion, where abundant callus formation or altered clavicular length likely contributed to vessel compression or erosion [9]. In other cases, a fixation screw had perforated a nearby vessel. Screw prominence following clavicle fixation has been particularly implicated as a risk factor for delayed vascular injury. In a case report by Clitherow and Bain five cases of vascular complications after clavicle fixation were identified, including four pseudoaneurysms and one arteriovenous fistula, with pseudoaneurysm presentation ranging from 2 to 10 years post-operatively [10]. In the three cases where measurements were available, screw prominence varied slightly from 8–10 mm. Of important note, three patients developed limb-threatening ischaemia. These findings highlight that even minimal hardware prominence has the potential to cause clinically significant vascular injury over extended periods of time. The anatomic proximity of the subclavian vessels to the clavicle likely plays a factor in this risk. As the subclavian artery and vein exit the thoracic cavity, they course in close relation to the medial two-thirds of the clavicle, separated by the scalenus anterior muscle before traversing the thoracic outlet and passing over the first rib. Anatomical studies have found that the subclavian vein is typically within 5 mm of the undersurface of the medial half of the clavicle, posing the greatest risk of all vasculature during clavicle injury and subsequent fixation. The subclavian artery generally lies deeper, with mean distances >20 mm, but can still be reported as little as 10 mm away medially depending on the side and individual anatomy [3]. Consistent with this, Chalidis et al. reported that subclavian vessel injury is an underestimated yet serious complication of displaced clavicle fractures, highlighting the importance of restoring length and alignment to reduce the risk of vascular compromise [1]. Neurovascular complications in clavicle fracture non-unions further support the need for clinical vigilance. Berkheiser reported brachial plexus involvement in six cases of clavicle non-union, while Ghormley identified both brachial plexus compression and subclavian vein obstruction in a series of 20 non-unions [11,12]. Although other series, such as that by Neer, reported no neurovascular complications in 18 cases, this variability in reported incidence underscores the need to maintain a high index of suspicion [13]. This is particularly true for patients with persistent supraclavicular masses, new or progressive neurologic deficits, or evolving signs of venous or arterial compromise. Systematic reporting of such complications is crucial to determine true incidence estimates, clarify risk factors and mechanisms, and ultimately guide evidence-based decisions regarding surveillance, timing of intervention, and surgical technique in patients like the one described in this case report. This case report is notable for several reasons and is unlike many previously stated cases. This patient had a well-healed clavicle without non-union, malunion, or hardware prominence, and imaging did not reveal direct screw impingement on the subclavian vessels. In addition, nearly 7 years after fracture fixation, the pseudoaneurysm presented and masqueraded as a supraclavicular mass and ultimately led to surgical biopsy before vascular diagnosis. This highlights that clinically significant vascular complications may occur even without the presence of classic radiographic risk factors.
A subclavian artery pseudoaneurysm is a rare but potentially life-threatening complication of clavicle fracture and surgical fixation and may result in a delayed or insidious fashion. This case demonstrates that vascular injury can occur even in the setting of a well-healed fracture without hardware prominence and may disguise itself as a benign supraclavicular mass. Persistent or unexplained supraclavicular swelling, exertional neurologic symptoms, or vascular findings in patients with a history of clavicle fracture or fixation should prompt early vascular imaging. Having a high index of suspicion is crucial to avoid delayed diagnosis and prevent catastrophic complications.
Clavicle fractures are one of the most common fractures seen by orthopaedic surgeons and are considered healed after confirming fixation and stabilisation. However, like in this case, delayed vascular complications may develop years after. Subclavian artery pseudoaneurysms can be present as a supraclavicular mass without any fracture, non-union, malunion, or hardware prominence. Failure to recognise this complication can result in a misdiagnosis and potentially life-threatening haemorrhage. Clinicians evaluating patients with prior clavicle injury or fixation should have a high index of suspicion if patients present with this kind of mass and should pursue vascular imaging before invasive diagnostic procedures. Patients should also be informed of this risk pre-operatively of the original fixation so they can monitor the potential development of a mass and seek medical attention if necessary.
References
- 1. Chalidis B, Davitis V, Papadopoulos P, Pitsilos C. Subclavian vessels injury: An underestimated complication of clavicular fractures. World J Crit Care Med 2024;13:98579. [Google Scholar] [PubMed]
- 2. Bentley TP, Hosseinzadeh S. Clavicle fractures. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/nbk507892 [Last accessed on 2026 Feb 07]. [Google Scholar] [PubMed]
- 3. Steinmetz G, Conant S, Bowlin B, Hamilton J, Allen J, Stoner J, et al. The anatomy of the clavicle and its in vivo relationship to the vascular structures: A 2D and 3D reconstructive study using ct scans. J Orthop Trauma 2020;34:e14-9. [Google Scholar] [PubMed]
- 4. Cogburn J, Gilens JF, Khodaee M. Pseudoaneurysm of the subclavian artery as a delayed complication of a clavicle fracture. BMJ Case Rep 2023;16:e252430. [Google Scholar] [PubMed]
- 5. Raviraja A, Chandrashekar C, Roshan S, Srinivas J. Subclavian artery and vein injury following clavicle fracture due to blunt trauma. Inj Extra 2009;40:36-8. [Google Scholar] [PubMed]
- 6. Ropars M, Thomazeau H, Huten D. Clavicle fractures. Orthop Traumatol Surg Res 2017;103:S53-9. [Google Scholar] [PubMed]
- 7. Pradel S, Brunaud M, Coulomb R, Kouyoumdjian P, Marès O. Less than 1.5cm shortening in clavicle midshaft fracture has long-term functional impact. Orthop Traumatol Surg Res 2023;109:103590. [Google Scholar] [PubMed]
- 8. Graham JM, Feliciano DV, Mattox KL, Beall AC Jr., DeBakey ME. Management of subclavian vascular injuries. J Trauma 1980;20:537-44. [Google Scholar] [PubMed]
- 9. Borole A, Vitkovska D, Yang J, Avendano JP, Monica J, Katt BM. Neurovascular complications following clavicle fracture fixation: Timing, mechanisms, and clinical implications. Cureus 2024;16:e74512. [Google Scholar] [PubMed]
- 10. Clitherow HD, Bain GI. Association between screw prominence and vascular complications after clavicle fixation. Int J Shoulder Surg 2014;8:122-6. [Google Scholar] [PubMed]
- 11. Berkheiser: Old Ununited Clavicular Fractures in the Adult. Available from: https://scholar.google.com/scholar_lookup?journal=Surg%20Gynecol%20Obstet&title=Old%20ununited%20clavicular%20fractures%20in%20the%20adult&author=E.%20J.%20Berkheiser&volume=64&publication_year=1937&pages=1064-1072& [Last accessed on 2026 Feb 07]. [Google Scholar] [PubMed]
- 12. Ghormley RK, Black JR, Cherry JH. Ununited fractures of the clavicle. Am J Surg 1941;51:343-9. [Google Scholar] [PubMed]
- 13. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc 1960;172:1006-11. [Google Scholar] [PubMed]
- 14. Howard FM, Shafer SJ. Injuries to the clavicle with neurovascular complications. A study of fourteen cases. J Bone Joint Surg Am 1965;47:1335-46. [Google Scholar] [PubMed]
- 15. Pairolero PC, Walls JT, Payne WS, Hollier LH, Fairbairn JF 2nd. Subclavian-axillary artery aneurysms. Surgery 1981;90:757-63. [Google Scholar] [PubMed]
- 16. Mellière D, Becquemin JP, Danis RK, Moretti JL. Reliability and value of arterial blood-flow monitoring during operation. J Mal Vasc 1981;6:129-32. [Google Scholar] [PubMed]
- 17. Coulier B, Mairy Y, Etienne PY, Joris JP. Late diagnosis of a traumatic pseudo-aneurysm of the subclavian artery. J Belge Radiol 1996;79:26-8. [Google Scholar] [PubMed]
- 18. Johnson B, Thursby P. Subclavian artery injury caused by a screw in a clavicular compression plate. Cardiovasc Surg 1996;4:414-5. [Google Scholar] [PubMed]
- 19. Casselman F, Vanslembroek K, Verougstraete L. An unusual cause of thoracic outlet syndrome. J Trauma 1997;43:142-3. [Google Scholar] [PubMed]
- 20. Serrano JA, Rodríguez P, Castro L, Serrano P, Carpintero P. Acute subclavian artery pseudoaneurysm after closed fracture of the clavicle. Acta Orthop Belg 2003;69:555-7. [Google Scholar] [PubMed]
- 21. Shackford SR, Connolly JF. Taming of the screw: A case report and literature review of limb-threatening complications after plate osteosynthesis of a clavicular nonunion. J Trauma 2003;55:840-3; discussion 843. [Google Scholar] [PubMed]
- 22. Rodriguez-Merchan EC, Gomez-Cardero P. Delayed union of a fracture of the middle third of the clavicle presenting with a late subclavian pseudoaneurysm. Musculoskelet Surg 2010;94:89-92. [Google Scholar] [PubMed]
- 23. Prater S, Marichal DA, Rees C. Endovascular management of suprascapular artery pseudoaneurysm. Proc Bayl Univ Med Cent 2010;23:24-6. [Google Scholar] [PubMed]
- 24. Bain GI, Galley IJ, Keogh AR, Durrant AW. Axillary artery pseudoaneurysm after plate osteosynthesis for a clavicle nonunion: A case report and literature review. Int J Shoulder Surg 2010;4:79-82. [Google Scholar] [PubMed]
- 25. Derom A, Ottenheim S, Raat H, Van Kleef J. Endovascular treatment of acute subclavian pseudo-aneurysm after fracture of the clavicle. Acta Chir Belg 2008;108:441-3. [Google Scholar] [PubMed]
- 26. Pallett SJ, Singh I, Rady N, Goshai H. Delayed subclavian artery aneurysm following fixation of a clavicular fracture. Vasc Endovascular Surg 2018;52:459-62. [Google Scholar] [PubMed]
- 27. Lewis SD, Chew FS. Clavicle fixation screw impingement causing subclavian artery pseudoaneurysm. Radiol Case Rep 2019;14:1148-50. [Google Scholar] [PubMed]
- 28. Belmir H, Chagou A, Tijani Y, Azghari A. Pseudoaneurysm of the subclavian artery following clavicle fracture due to blunt traumatism: A case report. Pan Afr Med J 2020;36:262. [Google Scholar] [PubMed]
- 29. Isse HM, Mohamed YG, Sereke SG, Valeria N. Iatrogenic giant subclavian artery pseudoaneurysm following clavicle fracture repair: A case report. Radiol Case Rep 2023;18:2339-42. [Google Scholar] [PubMed]
- 30. Lawson J, Crockett S, Griffiths D, Riga C, Sabharwal S, Thomas R, et al. Ruptured subclavian artery pseudoaneurysm following a shoulder massage on a background of clavicle non-union. BMJ Case Rep 2023;16:e253826. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report
November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report June 18, 2021 A Rare Case of Pseudoaneurysm of the Brachial Artery in Supracondylar Humerus Fracture
June 18, 2021 A Rare Case of Pseudoaneurysm of the Brachial Artery in Supracondylar Humerus Fracture June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report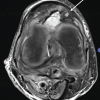 April 1, 2026 Pseudoaneurysm of the Medial Genicular Artery as a Rare Cause of Recurrent Knee Swelling – A Case Report
April 1, 2026 Pseudoaneurysm of the Medial Genicular Artery as a Rare Cause of Recurrent Knee Swelling – A Case Report