
X-rays of the blunt injury of the hand are a must, as the phalanges can get fractured easily. Differentiation between arterial ischaemia and venous congestion is important. In threatened ischaemia, the decision between surgery and conservative management has to be taken by serially monitoring the finger.
Dr. Balasubramanian Nellaiyappan, Department of Hand Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: drvenkatesh_11@hotmail.com
Abstract
Introduction: Paediatric crush injuries of the hand may present with fractures and threatened digital vascularity, requiring careful differentiation between venous congestion and arterial ischaemia.
Case Report: A 6-year-old boy sustained a crush injury to the left hand with phalangeal fractures and threatened vascularity of the middle finger. The patient was managed conservatively with immobilisation, limb elevation, hydration, anticoagulation, thermal support, and serial vascular monitoring. Progressive recovery of perfusion and viability was achieved without surgical intervention.
Conclusion: Conservative management with close observation may successfully salvage borderline ischaemic digits in selected paediatric crush injuries and avoid unnecessary surgical exploration.
Keywords: Pediatric crush injury, digital ischemia, venous congestion, missed injuries, precarious viability, deformity, stiffness.
Hand injuries are common in the paediatric population and may present with associated vascular compromise [1]. Crush injuries, in particular, can result in soft-tissue damage, fractures, and threatened digital viability [2]. While surgical intervention is often considered in cases of ischaemia, selected cases have to be managed conservatively with close monitoring and intervened in only when necessary because the surgical procedure per se can worsen the ischaemia. We report a case of a 6-year-old male child with a crush injury to the left hand presenting with venous congestion and threatened viability of the middle finger, along with phalangeal fractures. (Fig. 1)

Figure 1: Initial clinical image showing dusky middle finger with venous congestion.
The patient was managed with immobilisation, limb elevation, anticoagulation, and serial monitoring. Despite initial severe symptoms, gradual improvement in vascularity was observed, and the digit was successfully salvaged without surgical intervention. (Figs. 2 & 3).

Figure 2: Radiographs (Anteroposterior and lateral views) showing fractures of the middle finger.

Figure 3: Clinical progression showing improvement in vascularity.
This case highlights the importance of careful clinical assessment and emphasises that conservative management can be a viable option in paediatric patients with borderline digital ischaemia [3]. Phalangeal fractures account for a significant proportion of hand injuries, especially in children [1,4]. Most stable fractures can be managed conservatively; however, crush injuries often present with associated soft-tissue damage and vascular compromise, making management more challenging [2,5]. Digital ischaemia is a critical concern, as delayed or inappropriate management may result in tissue necrosis and permanent functional loss [6]. While surgical exploration is indicated in clear cases of arterial insufficiency, the management of borderline ischaemia and venous congestion remains controversial [7,8]. Paediatric patients possess a rich collateral circulation, which may allow recovery even in cases of initially compromised vascularity [3,9]. This case demonstrates successful conservative management of a child with threatened digital ischaemia of the middle finger following crush injury.
A 6-year-old male child presented with a history of an accidental fall off a study desk while playing at school and sustained injury to his left hand. The injury occurred due to direct compression of the hand. He immediately received treatment at a peripheral health centre and was managed conservatively, advised rest and ice pack application and sent home. However, X-rays of the finger were not taken. Patient attendees continued to notice there was a gradual increase in swelling and discolouration of the middle finger. Later, he was taken to another hospital where an orthopaedic surgeon ordered an X-ray, and the X-ray showed a comminuted phalangeal head fracture of the proximal phalanx of the middle finger. Due to the suspicious nature of the injury and darkish discolouration of skin, a suspected vascular injury, the patient had been referred to our tertiary care centre to the hand surgery unit (Sri Ramachandra Institute of Higher Education and Research). The patient had intact arterial flow and venous congestion and had been started on supportive measures such as a hand warmer, hydration, limb elevation, and medical management such as analgesics and low molecular weight heparin. There was no significant past medical or surgical history. Developmental milestones and immunisation status were appropriate for age.
Clinical examination:
On local examination, the left middle finger showed diffuse swelling and tenderness over the phalanges. The fingertip was cold to the touch with discolouration extending from the tip up to the proximal interphalangeal joint. Sensations were altered over the middle finger. Active range of motion (ROM) could not be assessed due to pain. The findings were suggestive of venous congestion with threatened digital ischaemia.
Imaging:
Radiographs (antero-posterior and lateral views) of the left hand revealed:
- Fracture of the head of the proximal phalanx of the middle finger
- Fracture at the base of the middle phalanx of the middle finger.
Management and hospital course:
The patient was admitted for close monitoring. Parents were counselled regarding the role of conservative management for venous congestion, the possibility of deterioration, and the potential need for surgical intervention, including amputation if the finger became non-viable. The patient was managed conservatively with:
- Immobilization using plaster of Paris below-elbow dorsal slab with wrist in neutral position and metacarpophalangeal joints in 90° flexion
- Hydration
- Low molecular weight heparin
- Limb elevation
- Serial monitoring of vascular status
- Analgesics and supportive care
- Hand therapy exercises
- Hand warmer.
Hospital course:
- Day 1: Late presentation, delayed diagnosis, severe pain and agitation; finger appeared dusky with marked venous congestion on arrival
- Day 2: Supportive measures augmented, and the finger continued to be precariously viable without any further worsening or improvement
- Day 3: No further worsening of symptoms (ray of hope in the air)
- Day 5: A significant level of recovery and marked improvement noticed
- Day 7: Progressive improvement in colour, warmth, and perfusion noted. Blister formation noted around the finger, and sterile evacuation done
- Day 12: Finger ROM initiated and therapy taught to the patient
- Day 14: Patient discharged from hospital with a further plan of operative skeletal stabilisation after a week.
The patient showed steady recovery and was discharged after 14 days with a viable middle finger. (Fig. 4).

Figure 4: Final outcome at discharge.
At the time of discharge, the middle finger showed the following:
- Restoration of vascularity
- Improved skin color and temperature
- Significant reduction in pain. The digit was successfully salvaged without surgical intervention.
The patient was advised for review, but the patient did not come as advised. No further treatment has been attempted for fracture management. The child continued to heal with a flexed posture of the proximal interphalangeal joint and started using his hand 3 months from the date of injury. Patient attendees had been contacted over the phone and advised to follow up, and we requested clinical images through the phone. The patient’s attenders shared a clinical image through the phone in WhatsApp but conveyed they were not interested in further intervention for the finger. (Fig. 5).
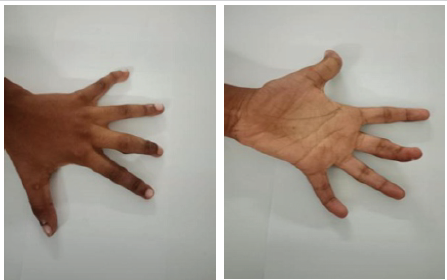
Figure 5: One-year follow-up shows with deformity of the finger, and assessment is limited due to non-availability of physical examination, as they were subjectively satisfied with the functional outcome.
During one year followup description
Crush injuries to the hand can result in both skeletal and vascular compromise. In paediatric patients, the presence of a robust collateral circulation increases the potential for recovery even in cases of threatened ischaemia [10,11]. Paediatric patients possess excellent collateral circulation and tissue healing potential compared with adults. Even digits that initially appear poorly perfused may recover with careful observation, elevation, splintage, and serial neurovascular monitoring [10,12]. Crush injuries of the hand are unique because the extent of vascular and soft-tissue damage is often underestimated during the initial examination. Progressive oedema and venous congestion may worsen tissue perfusion during the first 24–48 h, making repeated clinical assessment essential [11,13]. Conservative management can be considered in selected cases of borderline digital ischaemia where capillary refill gradually improves and no definite arterial transection is identified. Avoiding unnecessary surgical exploration may prevent additional trauma to already compromised tissues [10,13]. Early immobilisation and elevation play a significant role in reducing oedema and venous congestion in paediatric hand trauma. Reduction in swelling improves microvascular circulation and may aid spontaneous recovery of threatened digits [11,14]. Serial documentation of colour changes, temperature, capillary refill, oxygen saturation, and progression of swelling is essential in conservative management. Any deterioration in vascularity should prompt urgent reassessment for surgical intervention [13,14]. Functional recovery in children is generally superior because of rapid bone healing and adaptability of the growing hand. However, delayed stiffness, nail deformity, growth disturbances, and joint contracture may occur, highlighting the need for long-term follow-up and physiotherapy [14,15]. The present case supports the principle that not all congested or poorly perfused digits require immediate operative exploration. Careful patient selection and close monitoring may result in successful salvage with preservation of function and avoidance of unnecessary surgery [10,13]. Venous congestion may present with discolouration and swelling, often mimicking arterial insufficiency. However, it does not always indicate irreversible ischaemia. Differentiating between these conditions is essential to avoid unnecessary surgical intervention [13,16]. Conservative management, including limb elevation, anticoagulation, thermal support, and physiotherapy, can promote vascular recovery in selected cases [11,14]. Previous studies have demonstrated that while surgical fixation is necessary in unstable fractures, conservative management remains effective in carefully selected patients [11,15]. This case highlights the importance of serial clinical assessment and cautious decision-making, particularly in paediatric patients, where tissue recovery potential is high [10,12].
Limitations:
- This is a single case report, limiting the generalizability of the findings to broader pediatric populations
- Absence of a control or comparison group prevents direct comparison between conservative and surgical management outcomes
- The exact degree of arterial compromise could not be objectively quantified
- Advanced vascular imaging, such as Doppler ultrasonography or angiography, was not performed
- Pulse oximetry measurements of the affected digit were not documented serially
- Lack of objective perfusion assessment tools may limit reproducibility of decision-making
- The diagnosis of venous congestion versus arterial ischemia was based predominantly on clinical examination
- Delayed initial diagnosis at the peripheral center may have influenced the clinical course and outcomes
- The patient presented after prior treatment elsewhere, limiting assessment of the immediate post-injury status
- The exact timing and severity of vascular compromise progression could not be precisely determined
- Long-term follow-up was incomplete because the patient was lost to regular follow-up
- Final functional outcomes, such as grip strength, dexterity, and fine motor function, were not objectively assessed
- Long-term complications, including growth disturbances, stiffness, or physeal injury, could not be evaluated adequately
- Radiological union and long-term fracture remodeling were not fully documented
- Skeletal stabilization of the fractures was ultimately not performed, limiting assessment of fracture management outcomes
- Follow-up clinical assessment relied partly on telephonic communication and photographs shared through messaging applications
- The quality and accuracy of remotely shared clinical images may not reliably reflect true functional recovery
- Rehabilitation compliance and home-based physiotherapy adherence could not be objectively monitored
- Conservative management success in this case may not be applicable to patients with complete arterial disruption or severe crush injuries
Larger prospective studies are required to establish standardised protocols for differentiating venous congestion from threatened arterial ischaemia and to define indications for conservative versus surgical management in paediatric crush injuries.
Conservative management can be an effective treatment option in paediatric crush injuries with threatened digital ischaemia, provided close monitoring is ensured.
Paediatric crush injuries with threatened digital vascularity require careful serial assessment, as selected cases may recover successfully with conservative management and close monitoring. This case emphasises that not all cases of vascular compromise require immediate surgical intervention, and favourable outcomes can be achieved with appropriate non-operative care.
References
- 1. Nellans KW, Chung KC. Pediatric hand fractures. Hand Clin 2013;29:569-78. [Google Scholar] [PubMed]
- 2. Friedrich JB, Vedder NB. Hand crush injuries. J Am Academy Orthop Surg 2010;18:355-62. [Google Scholar] [PubMed]
- 3. Strauch B, De Moura W. Arterial system of the fingers. J Hand Surg 1990;15:148-54. [Google Scholar] [PubMed]
- 4. Cornwall R, Ricchetti ET. Pediatric phalanx fractures. J Hand Surg 2006;31:1720-31. [Google Scholar] [PubMed]
- 5. Abzug JM, Kozin SH. Pediatric hand trauma. Orthop Clin North Am 2014;45:545-59. [Google Scholar] [PubMed]
- 6. Higgins JP. Digital replantation and revascularization. J Hand Surg 2011;36:1108-12. [Google Scholar] [PubMed]
- 7. Sebastin SJ, Chung KC. Management of acute finger ischemia. Hand Clin 2015;31:23-34. [Google Scholar] [PubMed]
- 8. Goldfarb CA, Steffen JA. Acute vascular injuries of the hand. Hand Clin 2018;34:45-56. [Google Scholar] [PubMed]
- 9. Fufa DT, Chuang SS, Yang JY. Microvascular considerations in pediatric hand injuries. Clin Plastic Surg 2014;41:543-53. [Google Scholar] [PubMed]
- 10. Bougie E, Cugno S. Closed digital artery injury in children: A case report and review of the literature. Pediatr Emerg Care 2020;36:e233-5. [Google Scholar] [PubMed]
- 11. Sabapathy SR, Midgley RD, Moran SL, Peng YP, Soucacos PN, Buchler U, Kastaros J et al. Guidelines for management of crush injuries of the hand. J Clin Orthop Trauma 2020; [Google Scholar] [PubMed]
- 12. Loewenstein SN, Adkinson JM. Pediatric fingertip injuries. Hand Clin 2021;37:107-16. [Google Scholar] [PubMed]
- 13. Ahmad RS, Heng PR. Crush Injuries of the Hand Part II: Clinical Assessment, Management and Outcomes. London: IntechOpen; 2018. [Google Scholar] [PubMed]
- 14. Goodman A, Got CJ, Weiss AP. Crush injuries of the hand. J Hand Surg 2017;42:456-63. [Google Scholar] [PubMed]
- 15. Venkatesh A, Khajuria A, Greig AV. Management of pediatric distal fingertip injuries: A systematic literature review. Plast Reconstr Surg Glob Open 2019;8:e2595. [Google Scholar] [PubMed]
- 16. Pediatric Orthopaedic Society of North America. Pediatric Hand Trauma Guidelines. United States: Pediatric Orthopaedic Society of North America; [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture
August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture April 1, 2026 Total Talus Replacement using a Custom 3D-Printed Titanium Implant for Post-Traumatic Avascular Necrosis of Talus following Failed Internal fixation: A Case Report
April 1, 2026 Total Talus Replacement using a Custom 3D-Printed Titanium Implant for Post-Traumatic Avascular Necrosis of Talus following Failed Internal fixation: A Case Report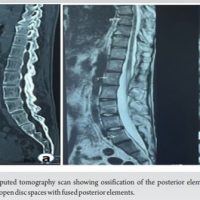 April 10, 2024 Utility of Asymmetric Multilevel Pontes Osteotomy in Ankylosing Spondylitis with Scoliosis using Ultrasonic Bone Scalpel: Case Report
April 10, 2024 Utility of Asymmetric Multilevel Pontes Osteotomy in Ankylosing Spondylitis with Scoliosis using Ultrasonic Bone Scalpel: Case Report May 10, 2023 Swan Neck Deformity: An Unusual Complication Following Trigger Finger Release
May 10, 2023 Swan Neck Deformity: An Unusual Complication Following Trigger Finger Release