
Cortical window osteotomy can provide safe and adequate tissue access for biopsy and curettage in deep-seated iliac osteomyelitis while preserving pelvic stability through anatomical reconstruction.
Dr. Chirag Sharma, Department of Orthopaedics, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India. E-mail: chiragammu@gmail.com
Abstract
Introduction: Iliac osteomyelitis is a rare and often overlooked condition because of its deep anatomical location and vague clinical presentation. Patients commonly present with persistent groin or pelvic pain and minimal systemic symptoms, frequently resulting in delayed diagnosis. Obtaining adequate tissue for microbiological and histopathological evaluation in such deep-seated lesions can also be challenging. We report a case of subacute iliac osteomyelitis managed using a cortical window osteotomy technique for diagnostic biopsy and curettage.
Case Report: A 19-year-old male presented with a 6-month history of progressively worsening right groin pain associated with intermittent low-grade fever and difficulty in walking. Laboratory investigations revealed elevated inflammatory markers. Magnetic resonance imaging demonstrated marrow oedema and cortical irregularity involving the right ilium with extension into the iliacus muscle, suggestive of subacute osteomyelitis. Computed tomography further defined the cortical involvement and assisted in surgical planning. Considering the deep location of the lesion and the need for adequate tissue sampling, an open biopsy was performed using a cortical window osteotomy approach. A hinged cortical flap was created to access the lesion, allowing curettage and collection of multiple tissue samples. The cortical segment was subsequently repositioned and fixed with cortical screws. Although microbiological investigations were negative, histopathology showed chronic inflammatory changes. The diagnosis was supported by the radiological findings, intraoperative appearance, elevated inflammatory markers, and the patient’s favourable clinical response to treatment. At follow-up, the patient had complete resolution of symptoms with maintained pelvic stability.
Conclusion: Cortical window osteotomy provided safe and satisfactory exposure for biopsy and curettage in this case while preserving pelvic integrity through anatomical reconstruction of the cortical segment. This technique may serve as a useful alternative in selected deep-seated iliac lesions where percutaneous biopsy is unlikely to provide adequate tissue.
Keywords: Iliac osteomyelitis, cortical osteotomy, pelvic osteomyelitis, bone biopsy, subacute osteomyelitis.
Pelvic osteomyelitis is an uncommon but clinically significant form of musculoskeletal infection, accounting for approximately 1–11% of cases of haematogenous osteomyelitis [1]. Among pelvic sites, involvement of the ilium is particularly challenging because of its deep anatomical location and the often non-specific nature of presenting symptoms [2]. As a result, diagnosis is frequently delayed, especially in adolescents and young adults who may initially present only with vague groin pain, limp, or intermittent fever [2]. Subacute osteomyelitis represents a more indolent form of infection and is commonly associated with low-virulence organisms or prior partial antibiotic exposure [3]. The absence of overt systemic features can further obscure the diagnosis. In tuberculosis-endemic regions such as India, tubercular osteomyelitis must also be carefully considered in the differential diagnosis of destructive iliac lesions [4]. Magnetic resonance imaging (MRI) plays a pivotal role in early diagnosis because of its high sensitivity in detecting marrow oedema, soft-tissue extension, and abscess formation [5]. Computed tomography (CT) complements MRI by providing superior delineation of cortical destruction and aiding pre-operative planning [5]. Despite advances in imaging, however, definitive diagnosis still depends on obtaining adequate tissue for microbiological and histopathological evaluation [5]. The ideal biopsy approach for iliac osteomyelitis remains uncertain. CT-guided percutaneous biopsy is minimally invasive but may provide insufficient tissue, particularly in necrotic or heterogeneous lesions [6]. Conventional open approaches allow direct visualisation and more extensive sampling, although they may be associated with greater surgical morbidity and increased soft-tissue disruption [6]. Consequently, there remains a need for techniques that permit adequate tissue sampling while preserving pelvic stability and minimising structural damage. Cortical window osteotomy techniques have previously been described in the management of Brodie’s abscess and other forms of subacute osteomyelitis involving long bones [7]. These methods allow direct access to the lesion while preserving cortical continuity through replacement of the cortical segment following curettage. However, their application in iliac osteomyelitis has rarely been discussed in the literature. We report a case of subacute iliac osteomyelitis in a young adult managed using a posterior iliac cortical osteotomy technique for diagnostic biopsy and curettage. The approach provided satisfactory exposure for tissue sampling while preserving pelvic integrity and may represent a useful alternative in selected cases.
A 19-year-old male presented to the outpatient department with a 6-month history of progressively worsening right groin pain associated with intermittent low-grade fever and mild limitation in walking distance. There was no history of trauma, antecedent skin infection, sinus formation, or significant systemic illness. One month before presentation, he had been evaluated at a peripheral healthcare facility and treated symptomatically with analgesics, without meaningful improvement. On examination, the patient was afebrile and haemodynamically stable. General physical examination and anthropometric assessment were unremarkable. Local examination revealed deep-seated tenderness over the right iliac crest and inner aspect of the iliac fossa. No erythema, local warmth, fluctuation, or sinus tract was noted. Hip range of motion was preserved in all planes, and passive rotational movements were painless, suggesting that the hip joint itself was not the primary source of pathology. Distal neurovascular examination of the affected limb was normal. Laboratory investigations demonstrated elevated inflammatory markers, including erythrocyte sedimentation rate and C-reactive protein. Total leukocyte count was mildly elevated with neutrophilic predominance. Blood cultures were obtained but showed no microbial growth. Plain anteroposterior radiographs of the pelvis were largely unremarkable, with preserved bilateral hip joint spaces and no obvious osteolytic or sclerotic lesion involving the ilium. On closer inspection, subtle haziness over the right iliac region was appreciated, although this was non-specific (Fig. 1 and 2).

Figure 1: Pre-operative anteroposterior radiograph of the pelvis demonstrating preserved bilateral hip joint spaces without an obvious destructive lesion.
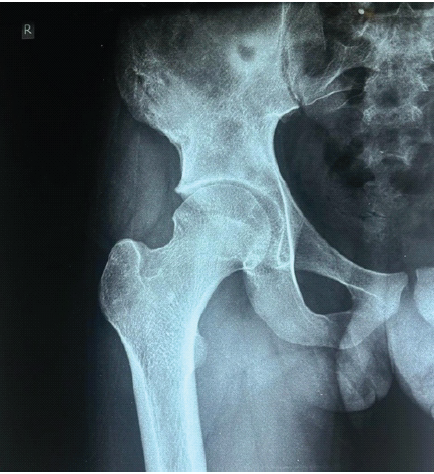
Figure 2: Focused radiograph of the right hemipelvis demonstrating subtle haziness and cortical irregularity involving the right ilium.
Subsequent MRI of the pelvis demonstrated marrow oedema and cortical irregularity involving the right ilium, along with extension into the iliacus muscle, findings suggestive of subacute osteomyelitis with adjacent soft-tissue involvement (Fig. 3).
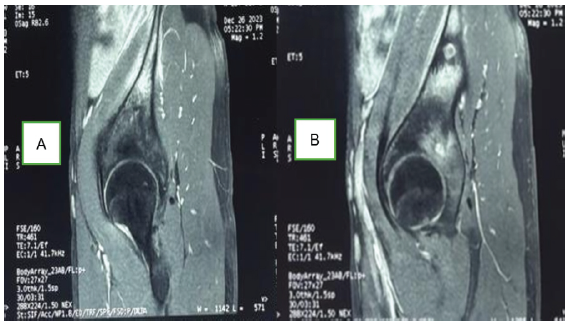
Figure 3: (a) Sagittal magnetic resonance imaging section demonstrating marrow edema and cortical irregularity involving the right ilium. (b) Adjacent sagittal section showing extension of inflammatory changes into the adjacent iliacus musculature and surrounding soft tissues.
CT further delineated cortical involvement and aided preoperative planning. The femoral heads demonstrated preserved sphericity and normal marrow signal bilaterally, with no radiological evidence of hip joint involvement. In view of the deep-seated nature of the lesion and the need for adequate tissue sampling, an open biopsy was planned following routine pre-operative evaluation and anaesthetic clearance.
Technical note in cortical window osteotomy:
Under general anaesthesia, the patient was positioned in the lateral decubitus position with the affected side up and appropriately padded. A anterior iliac approach was utilised. A 6 cm incision was made parallel to the iliac crest, centred over the region corresponding to maximal abnormality as noted in MRI images. Following division of the fascia, the musculature was elevated subperiosteally to expose the outer table of the ilium. A rectangular cortical window measuring approximately 3 × 4 cm was created using an oscillating saw while preserving a periosteal hinge on the cranial side, thereby allowing elevation of the cortical segment as a flap. The cortical window was carefully reflected, and two Hohmann retractors were carefully placed to expose the lesion. An intraoperative X-ray was taken to confirm and localise the lesion. On entering the lesion, necrotic granular tissue with a purulent appearance was encountered and thoroughly curetted.
Multiple tissue samples were obtained in separate sterile containers and sent for aerobic, anaerobic, and fungal culture; cartridge-based nucleic acid amplification test (CB-NAAT) (Xpert Mycobacterium tuberculosis complex/resistance to rifampin assay); and histopathological examination, including haematoxylin and eosin and Ziehl–Neelsen staining. Following thorough saline lavage, the cortical flap was repositioned anatomically and secured using two 3.5 mm titanium cortical screws. Layered wound closure was performed, and a drain was placed and removed after 48 h. The post-operative period was uneventful. Empirical intravenous cefuroxime was administered perioperatively and later tailored according to microbiological findings. The wound healed satisfactorily by primary intention (Fig. 4).

Figure 4: Clinical post-operative photograph demonstrating a healed anterior iliac surgical incision without evidence of wound complications or sinus formation.
Microbiological investigations, including culture and CB-NAAT, were negative. Histopathological examination demonstrated fibrocollagenous tissue with chronic inflammatory cell infiltrates and granulation tissue formation, without evidence of granuloma, malignancy, or acid-fast bacilli. At the 2-week follow-up, the patient reported substantial improvement in pain and had no further febrile episodes. By 6 weeks, inflammatory markers had shown a declining trend, and the patient had resumed normal ambulation with a painless full range of hip motion. Follow-up radiographs demonstrated the maintained position of the cortical flap and stable screw fixation (Fig. 5).

Figure 5: Post-operative anteroposterior radiograph of the pelvis demonstrating anatomical repositioning of the anterior iliac cortical flap secured with two cortical screws over the right ilium, with maintained pelvic alignment and stable fixation.
Pelvic osteomyelitis remains an uncommon and diagnostically challenging condition because of its deep anatomical location, subtle clinical presentation, and frequently non-specific early imaging findings [1,2]. Delayed diagnosis is common, particularly in adolescents and young adults presenting with vague groin, hip, or lower abdominal pain without overt systemic features. In the present case, the patient experienced symptoms for nearly 6 months before a definitive diagnosis was considered, reflecting the indolent course often associated with subacute osteomyelitis. MRI plays a central role in the evaluation of suspected pelvic osteomyelitis because of its high sensitivity for detecting marrow oedema, cortical involvement, abscess formation, and soft-tissue extension [5]. In our patient, MRI clearly demonstrated involvement of the right ilium with extension into the iliacus muscle, a recognised pattern of spread in iliac osteomyelitis [2]. CT imaging further complemented these findings by better defining cortical destruction and assisting in surgical planning. In the present case, the deep-seated nature of the lesion and concern regarding inadequate sampling from necrotic tissue prompted an open biopsy approach. Obtaining a tissue diagnosis remains important in cases of suspected pelvic infection, particularly in tuberculosis-endemic settings where tubercular osteomyelitis must be excluded [4]. Nevertheless, microbiological confirmation is not always achieved. Previous studies have shown that blood cultures are positive in only 40–50% of cases of acute osteomyelitis, with even lower yields in subacute presentations [8]. Similarly, tissue cultures may remain negative despite clear radiological and intraoperative evidence of infection, especially following prior antibiotic exposure or in infections caused by low-virulence organisms [3,8]. In the present case, microbiological studies, including culture and CB-NAAT, were negative, whereas histopathology demonstrated only non-specific chronic inflammatory changes. Despite the absence of definitive microbiological confirmation, the diagnosis of osteomyelitis was supported by the characteristic imaging findings, intraoperative appearance of necrotic inflammatory tissue, elevated inflammatory markers, and subsequent clinical and biochemical improvement following treatment. Importantly, no histopathological evidence of malignancy or granulomatous disease was identified. Several biopsy techniques have been described for lesions involving the ilium and pelvis. CT-guided percutaneous biopsy offers the advantage of minimal invasiveness but may yield insufficient tissue, particularly in necrotic, heterogeneous, or deep-seated lesions [6,9]. Reported diagnostic yields vary considerably in the literature [9]. Conventional open approaches provide direct visualisation and allow more extensive debridement, although they may involve greater soft-tissue dissection and increased surgical morbidity [10]. The cortical window osteotomy technique has previously been described for the management of Brodie’s abscess and subacute osteomyelitis of long bones [7,11]. By creating a replaceable cortical window, the technique permits direct access to the lesion while preserving the structural continuity and biological activity of bone [12,13,14]. In addition to facilitating adequate curettage and tissue sampling, replacement of the cortical segment may help reduce dead space and maintain local stability. Its application in flat bones such as the ilium, however, has been rarely discussed. In our case, the posterior iliac cortical osteotomy approach provided safe, direct access to the lesion while avoiding major neurovascular structures associated with anterior pelvic approaches. The hinged cortical flap allowed adequate exposure for biopsy and curettage while enabling anatomical reconstruction following the procedure. We believe this technique offers a practical balance between adequate surgical access and preservation of pelvic integrity, particularly in selected cases where percutaneous biopsy may be inadequate. To our knowledge, reports specifically describing the use of a hinged posterior iliac cortical osteotomy for diagnostic biopsy in isolated iliac osteomyelitis remain limited in the literature. Although this is a single-case experience, the favourable clinical and radiological outcome observed in our patient suggests that the technique may represent a useful alternative approach in carefully selected patients. Reported outcomes in pelvic osteomyelitis are generally favourable when early diagnosis and appropriate surgical and antibiotic management are achieved, with success rates approaching 85–90% in some series [1,2]. Inflammatory markers typically normalise within 6–8 weeks in subacute disease [3], which was consistent with the clinical course observed in the present case.
Limitations:
This report describes a single patient, limiting the generalisability of the findings. Microbiological investigations, including culture and CB-NAAT, were negative, whereas histopathology showed only non-specific chronic inflammatory changes, preventing definitive etiological confirmation. Although the overall findings strongly supported osteomyelitis, other conditions, such as Ewing sarcoma or lymphoma, may occasionally mimic similar presentations. Follow-up duration was relatively short and did not allow long-term assessment of recurrence, cortical healing, functional outcomes, or implant-related complications. In addition, this technique may not be suitable for all iliac lesions and requires careful surgical planning and familiarity with pelvic anatomy. Further studies are required to evaluate its reproducibility, biomechanical stability, and long-term outcomes.
Iliac osteomyelitis is an uncommon and often under-recognised condition that should be considered in young patients presenting with persistent groin or pelvic pain associated with elevated inflammatory markers, even when initial radiographs appear normal. Early MRI plays an important role in establishing the diagnosis and defining the extent of the disease. Adequate tissue sampling remains essential for excluding alternative pathologies and guiding management, particularly in regions where tubercular infection is prevalent. The cortical window osteotomy technique described in this report provided satisfactory exposure for biopsy and curettage while preserving pelvic stability by anatomically replacing the cortical segment. This approach may represent a useful alternative in selected deep-seated iliac lesions where percutaneous biopsy is unlikely to yield adequate tissue and conventional open approaches may be associated with greater morbidity. Further experience and larger studies are required to better define its role in the management of pelvic osteomyelitis.
Cortical window osteotomy is a practical and structurally preserving technique that can facilitate adequate tissue sampling and curettage in selected cases of deep-seated iliac osteomyelitis.
References
- 1. Karimi A, Alborzi A, Rasooli M, Kadivar MR, Nateghian AR. Prevalence of causative agents of osteomyelitis in children: A hospital-based study. Arch Pediatr Adolesc Med 2009;163:561-5. [Google Scholar] [PubMed]
- 2. Longjohn DB, Zionts LE, Stott NS. Acute hematogenous osteomyelitis of the epiphysis. Clin Orthop Relat Res 1995;316:227-34. [Google Scholar] [PubMed]
- 3. Brodie BC. An account of some cases of chronic abscess of the tibia. Med Chir Trans 1832;17:239-49. [Google Scholar] [PubMed]
- 4. Mittal R, Gupta V, Rastogi S. Tuberculosis of the foot. J Bone Joint Surg Br 1999;81:997-1000. [Google Scholar] [PubMed]
- 5. Jaramillo D. Infection: Musculoskeletal. Pediatr Radiol 2011;41 Suppl 1:S127-34. [Google Scholar] [PubMed]
- 6. Pääkkönen M, Peltola H. Management of a child with suspected acute septic arthritis or osteomyelitis. Clin Infect Dis 2012;55:1485-91. [Google Scholar] [PubMed]
- 7. Schranz PJ, Vaishnav S. The cortical window technique in the treatment of Brodie’s abscess of the distal tibia. J Bone Joint Surg Br 1992;74:687-90. [Google Scholar] [PubMed]
- 8. Lew DP, Waldvogel FA. Osteomyelitis. Lancet 2004;364:369-79. [Google Scholar] [PubMed]
- 9. Skjeldal S, Norderval S. CT-guided percutaneous biopsy in musculoskeletal tumors and infections: A prospective study. Acta Orthop Scand 1994;65:432-6. [Google Scholar] [PubMed]
- 10. Hefti F. Paediatric Orthopaedics in Practice. 2nd ed. Berlin: Springer; 2007. p. 452-7. [Google Scholar] [PubMed]
- 11. Schranz PJ, Vaishnav S. Brodie’s abscess: A study of 33 cases treated with a cortical window technique. J Bone Joint Surg Br 1996;78:815-9. [Google Scholar] [PubMed]
- 12. Morrey BF, Bianco AJ Jr., Rhodes KH. Haematogenous osteomyelitis at uncommon sites in adults. Mayo Clin Proc 1978;53:707-13. [Google Scholar] [PubMed]
- 13. Hulkko A, Lanning P, Serlo W. Treatment of Brodie’s abscess with the cortical bone-window technique. Acta Orthop Scand 1989;60:438-40. [Google Scholar] [PubMed]
- 14. World Health Organization. Xpert MTB/RIF Assay for the Diagnosis of Pulmonary and Extrapulmonary TB in Adults and Children: Policy Update. Geneva: WHO; 2013. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Indolent Systemic Mastocytosis Presenting with Consecutive Vertebral Fragility Fractures despite Normal Bone Mineral Density: A Case Report and Mechanistic Review
May 1, 2026 Indolent Systemic Mastocytosis Presenting with Consecutive Vertebral Fragility Fractures despite Normal Bone Mineral Density: A Case Report and Mechanistic Review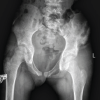 May 1, 2026 Methicillin-Resistant Staphylococcus aureus Iliac Osteomyelitis with Cortical Breach Mimicking Septic Arthritis of the Hip in a Child: A Diagnostic Pitfall
May 1, 2026 Methicillin-Resistant Staphylococcus aureus Iliac Osteomyelitis with Cortical Breach Mimicking Septic Arthritis of the Hip in a Child: A Diagnostic Pitfall October 1, 2024 Brodie’s Abscess of the Ankle Presenting as a Tumor: A Summary of Five Cases
October 1, 2024 Brodie’s Abscess of the Ankle Presenting as a Tumor: A Summary of Five Cases September 10, 2021 Brodie’s Abscess of the Proximal Humerus Metaphysis: A Case Report
September 10, 2021 Brodie’s Abscess of the Proximal Humerus Metaphysis: A Case Report