
Tuberculosis should be considered in the differential diagnosis of chronic elbow pain and swelling in immunocompromised patients, as early diagnosis and treatment can prevent joint destruction and improve outcomes.
Dr. S Harish Kiran, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: harishkiran.2694@gmail.com
Abstract
Introduction: Tuberculosis (TB) involving the elbow joint is an uncommon form of osteoarticular infection and often presents with non-specific symptoms, leading to delayed diagnosis and treatment. The condition may mimic other chronic inflammatory or infective arthropathies, posing significant diagnostic challenges. In patients with chronic kidney disease (CKD) undergoing hemodialysis, the presence of an arteriovenous (AV) fistula in the affected limb further complicates both clinical evaluation and surgical management. Reports describing TB of the elbow in the setting of CKD with an ipsilateral AV fistula are extremely limited, making this case clinically significant and relevant to orthopedic practice.
Case Report: A 75-year-old gentleman of South Indian origin presented with pain, swelling, and restricted movements of the left elbow of 2 weeks' duration, associated with intermittent low-grade fever. He was a known case of CKD on maintenance hemodialysis through an AV fistula in the same limb. Clinical examination revealed diffuse swelling, warmth, and tenderness around the elbow joint with restricted range of motion. Radiographs were unremarkable, while magnetic resonance imaging suggested joint effusion with surrounding soft-tissue involvement. The patient underwent surgical drainage and curettage following pre-operative optimization of the kidney function. Microbiological molecular testing confirmed TB with resistance to rifampicin, while histopathology showed features of chronic inflammation. The patient showed clinical improvement following surgical intervention and initiation of appropriate medical therapy.
Conclusion: This case highlights the importance of maintaining a high index of suspicion for TB in atypical presentations of elbow joint pathology, especially in immunocompromised individuals. The coexistence of CKD and an AV fistula presents unique diagnostic and therapeutic challenges, requiring a multidisciplinary approach. Early recognition and combined clinical, radiological, and laboratory evaluation are essential to prevent joint destruction and functional disability. This report contributes to orthopedic literature by emphasizing a rare clinical scenario and underscores the need for individualized management strategies in complex patients, thereby enhancing understanding of disease presentation and optimizing treatment outcomes.
Keywords: Tuberculosis, elbow joint, chronic kidney disease, arteriovenous fistula, septic arthritis.
Tuberculosis (TB) remains a major global health challenge, particularly in developing countries, with a high burden of both pulmonary and extrapulmonary disease. Despite advances in diagnosis and treatment, TB continues to cause significant morbidity and mortality worldwide, especially in endemic regions such as India. Musculoskeletal TB represents a small but clinically significant proportion of extrapulmonary TB, accounting for approximately 1–3% of total TB cases and up to 30–40% of extrapulmonary involvement [1,2]. Among these, extraspinal osteoarticular TB is relatively uncommon and often presents diagnostic challenges due to its indolent course and non-specific clinical features [3,4]. The elbow joint is a rare site of involvement in osteoarticular TB, constituting only 1–5% of musculoskeletal TB cases [2,5]. TB of the elbow typically presents as a chronic monoarthritis with a gradual onset of pain, swelling, and progressive restriction of joint movements. Constitutional symptoms such as fever, weight loss, and malaise may be absent or subtle, further complicating early recognition [5]. Due to its atypical presentation, elbow TB is frequently misdiagnosed as septic arthritis, rheumatoid arthritis, or other inflammatory arthropathies, resulting in delayed diagnosis and treatment [1,6]. Such delays can lead to irreversible joint destruction, deformity, and functional disability. Early diagnosis of osteoarticular TB is critical, as prompt initiation of antitubercular therapy can preserve joint integrity and improve functional outcomes. However, no single diagnostic modality is sufficiently sensitive or specific, necessitating a combination of clinical evaluation, radiological imaging, microbiological testing, and histopathological confirmation [2,7]. Advanced molecular diagnostic techniques, such as nucleic acid amplification tests, have improved the rapid detection of Mycobacterium tuberculosis, particularly in paucibacillary extrapulmonary forms [7]. The diagnostic and therapeutic challenges are further amplified in patients with chronic kidney disease (CKD) undergoing hemodialysis. These patients are immunocompromised and have an increased susceptibility to infections, including TB. In addition, the presence of an arteriovenous (AV) fistula, which serves as a critical vascular access for dialysis, introduces unique anatomical and surgical considerations. The fistula may obscure clinical findings, limit surgical approaches, and increase the risk of complications during invasive procedures [8]. Furthermore, altered pharmacokinetics in CKD necessitate careful dose adjustment of antitubercular drugs, complicating management strategies. There is limited literature addressing TB of the elbow in the setting of CKD with an ipsilateral AV fistula, making such cases rare and clinically significant. The coexistence of these conditions can lead to diagnostic ambiguity and therapeutic dilemmas, requiring a multidisciplinary approach involving orthopedics, nephrology, and infectious disease specialists [9,10]. This case report highlights the diagnostic challenges and management complexities of elbow TB in a patient with CKD and an AV fistula, emphasizing the importance of early suspicion, comprehensive evaluation, and individualized treatment strategies.
A 75-year-old male patient from South India presented with complaints of left elbow pain and swelling of 2 weeks’ duration. The onset was insidious, gradually progressive, and aggravated by movement, with no identifiable relieving factors. The patient also reported intermittent low-grade fever with evening rise for 6 days, associated with chills. There was no history of cough, weight loss, or loss of appetite. One day before admission, the patient developed altered sensorium. The patient was a known case of CKD stage V on maintenance hemodialysis for the past 5 years. He had undergone AV fistula creation in the left upper limb for vascular access. His comorbidities included systemic hypertension and Type 2 diabetes mellitus. There was no history of drug allergy or prior similar complaints. On general examination, the patient was afebrile with stable vital parameters. Pallor was present, while icterus, cyanosis, clubbing, lymphadenopathy, and pedal edema were absent. Systemic examination of the cardiovascular, respiratory, abdominal, and central nervous systems revealed no significant abnormalities. Local examination of the left elbow revealed a functioning AV fistula over the anterior aspect of the arm with a palpable thrill. Diffuse swelling was present around the elbow joint, associated with local warmth and diffuse tenderness. Passive range of motion was restricted to 80–110°, while active wrist and finger movements were preserved. Distal pulses were palpable, and sensory examination was intact (Fig. 1).
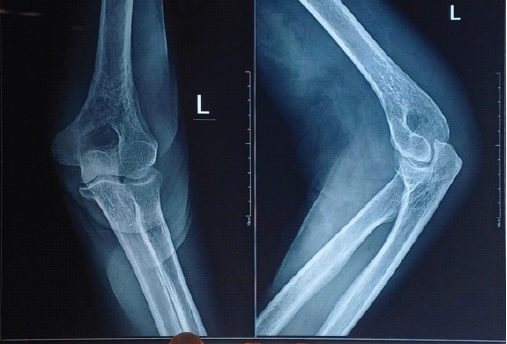
Figure 1: Plain radiograph of the left elbow (anteroposterior and lateral views) showing preserved joint alignment with no obvious fracture or gross bony destruction.
Laboratory investigations revealed elevated inflammatory markers, with erythrocyte sedimentation rate markedly raised and mildly elevated C-reactive protein levels. Renal function tests were deranged, consistent with CKD, with elevated serum creatinine and blood urea nitrogen levels. Hemoglobin was low, necessitating a blood transfusion during the hospital stay. Plain radiographs of the left elbow showed no evidence of fracture or obvious bony destruction. Magnetic resonance imaging (MRI) demonstrated synovial thickening with joint effusion involving the distal humerus and elbow joint, showing diffusion restriction suggestive of septic arthritis. Associated findings included myositis of the triceps and brachialis muscles, fasciitis around the elbow joint, cellulitis involving the distal arm and forearm, and a possible small intramuscular abscess (Fig. 2).
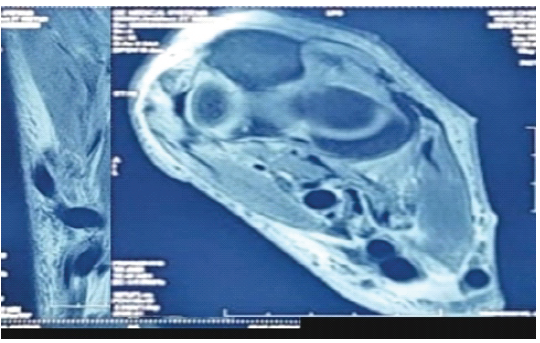
Figure 2: Magnetic resonance imaging of the left elbow demonstrating synovial thickening with joint effusion and surrounding soft-tissue involvement, suggestive of septic arthritis with associated myositis and possible intramuscular abscess formation.
Based on clinical and radiological findings, a provisional diagnosis of left elbow septic arthritis with possible osteomyelitis was made. After multidisciplinary evaluation and pre-operative optimization, including hemodialysis and correction of coagulation parameters with fresh frozen plasma, the patient underwent left elbow arthrotomy with drainage and distal humerus osteomyelitis curettage under regional nerve block anesthesia. Intraoperatively, tissue samples were collected for microbiological culture, molecular testing, and histopathological examination. Postoperatively, the patient underwent additional hemodialysis sessions and received a blood transfusion for anemia. Empirical antibiotic therapy was initiated and adjusted according to renal function. Microbiological culture showed no growth; however, molecular testing using GeneXpert detected M. tuberculosis with rifampicin resistance. Histopathological examination revealed dense acute-on-chronic inflammatory infiltrate composed of neutrophils, lymphocytes, and plasma cells, consistent with tubercular etiology. Following surgery, the patient showed clinical improvement with a reduction in pain and swelling. The surgical wound healed satisfactorily, and no post-operative complications were observed. The patient was started on antitubercular therapy under specialist guidance, with dose modifications according to renal status. Maintenance hemodialysis was continued thrice weekly through central venous access, with regular monitoring of renal and hepatic function (Fig. 3). On follow-up, the patient demonstrated gradual improvement in joint function with the initiation of gentle range of motion exercises, and no recurrence of symptoms was noted.

Figure 3: Post-operative clinical image of the left elbow showing a healed surgical incision with skin staples following arthrotomy and debridement.
Osteoarticular TB is a rare manifestation, accounting for only 1–3% of all TB cases, with elbow involvement being particularly uncommon, making this case clinically significant [11,12]. The uniqueness of this case lies in the coexistence of elbow TB with CKD on long-term hemodialysis and ipsilateral AV fistula, a combination rarely reported, where uremia-induced immune dysfunction predisposes to extrapulmonary TB [13,14]. Pathophysiologically, impaired cell-mediated immunity in CKD facilitates reactivation or dissemination of M. tuberculosis, often leading to atypical, localized musculoskeletal involvement without pulmonary features. Diagnostic challenges are significant, as osteoarticular TB presents insidiously with non-specific symptoms and often mimics septic arthritis or osteomyelitis, leading to delayed diagnosis and joint destruction [15,16]. An accurate diagnosis of TB is best achieved through an integrated approach that correlates clinical features with radiological, microbiological, and histopathological findings. Relying on these modalities improves diagnostic accuracy and helps confirm the presence and extent of disease. Non-invasive investigations mainly include imaging techniques such as plain radiography (X-rays), computed tomography (CT), positron emission tomography combined with CT, ultrasonography, and MRI. These modalities assist in identifying suggestive lesions, evaluating disease severity, and determining the anatomical extent of involvement. Invasive and laboratory-based investigations include hematological tests such as routine hemograms and immunological assessments like the Mantoux test and Interferon-Gamma Release Assays. Microbiological confirmation can be obtained through techniques like Ziehl-Neelsen staining, fluorescence microscopy, and culture of clinical specimens. Additionally, histopathological examination of tissue samples can demonstrate granulomatous inflammation, often with caseous necrosis, which supports the diagnosis. Recent advances in molecular diagnostics, particularly polymerase chain reaction–based assays such as GeneXpert, enable rapid identification of M. tuberculosis and provide information regarding potential drug resistance. Similar to our case, culture negativity is common, necessitating reliance on molecular diagnostics. GeneXpert has emerged as a highly sensitive and specific tool (sensitivity ~92% and specificity ~99%) for detecting TB and drug resistance even in culture-negative cases [17,18]. Literature supports combined surgical and medical management, especially in cases with abscess or joint involvement, with debridement improving outcomes [19]. Furthermore, drug-resistant TB, though uncommon, has been reported in osteoarticular cases, emphasizing the importance of early molecular testing [20]. Thus, this case underscores the need for high clinical suspicion, early biopsy, and advanced diagnostics in atypical presentations, particularly in immunocompromised patients (Fig. 2).
This case highlights the diagnostic and therapeutic challenges associated with TB of the elbow joint, particularly in elderly patients with multiple comorbidities such as CKD. The presence of an ipsilateral AV fistula further complicates both clinical evaluation and surgical management, often contributing to delayed diagnosis. The case reinforces the importance of maintaining a high index of suspicion for TB in atypical presentations of monoarthritis, especially in endemic regions. A combined approach involving clinical assessment, advanced imaging, and molecular diagnostic techniques is essential for early and accurate diagnosis. Surgical intervention, when indicated, must be carefully planned in the presence of vascular access devices. This case adds to existing literature by highlighting a rare clinical scenario and emphasizes the need for individualized, multidisciplinary management strategies to prevent joint destruction and optimize functional outcomes.
Tuberculosis should always be considered in chronic or atypical elbow joint infections, particularly in immunocompromised patients; early diagnosis and a multidisciplinary approach are crucial to prevent irreversible joint damage, especially in the presence of complicating factors such as an arteriovenous fistula.
References
- 1. Limaiem F, Gharbi MA, Bouhajja L, Bouzidi R. Tuberculous osteo-arthritis unmasked through unusual elbow swelling: A case report. Int J Surg Case Rep 2025;126:110759. [Google Scholar] [PubMed]
- 2. Upadhyaya GK, Kumar A, Iyengar KP, Agarwal A, Jain VK. Current concepts in the diagnosis and management of tuberculosis of the elbow joint. J Clin Orthop Trauma 2021;19:200-8. [Google Scholar] [PubMed]
- 3. Nouicer S, Jlidi M, Chaabane I, Bachrouch S, Tounsi H, Mallek K, et al. Extraspinal osteoarticular tuberculosis: A diagnostic and therapeutic challenge. Int J Mycobacteriol 2023;12:508-12. [Google Scholar] [PubMed]
- 4. Sequeira W, Co H, Block JA. Osteoarticular tuberculosis: Current diagnosis and treatment. Am J Ther 2000;7:393-8. [Google Scholar] [PubMed]
- 5. Dorji K, Wangchuk K, Choden S. Tuberculous arthritis in an adolescent’s elbow joint: A case report and literature review. Clin Case Rep 2025;13:e71236. [Google Scholar] [PubMed]
- 6. Manske J, Tille E, Schlüßler A, Biewener A, Nowotny J. Tuberculosis of the elbow joint: The complexity of diagnosis and treatment-a case report and review of literature. J Med Case Rep 2025;19:88. [Google Scholar] [PubMed]
- 7. Cataño J, Sanchez-Bautista J. Osteoarticular tuberculosis. Am J Trop Med Hyg 2022;106:1575-6. [Google Scholar] [PubMed]
- 8. Stegmayr B, Willems C, Groth T, Martins A, Neves NM, Mottaghy K, et al. Arteriovenous access in hemodialysis: A multidisciplinary perspective for future solutions. Int J Artif Organs 2021;44:3-16. [Google Scholar] [PubMed]
- 9. Liu Y, Wang X, Peng X, Lu L, Yang H, Feng G, et al. The epidemiology and disease economic burden of osteoarticular tuberculosis in hospitalized children in China: A nationwide cross-sectional retrospective study. BMC Infect Dis 20251;25:1377. [Google Scholar] [PubMed]
- 10. Wilmink J, Vollenberg R, Olaru ID, Fischer J, Trebicka J, Tepasse PR. Diagnostic challenges in extrapulmonary tuberculosis: A single-center experience in a high-resource setting at a German tertiary care center. Infect Dis Rep 2025;17:39. [Google Scholar] [PubMed]
- 11. Kumar S, Kumar R, Jayant N, Gautam C, Aggarwal V. Calcaneum tuberculosis-an uncommon phenomenon: Narrative review. Int J Res Orthop 2025;11:441-7. [Google Scholar] [PubMed]
- 12. Ramadugu R, Suvvari T, Ramadugu S, Temburu S, Srivastava D. A rare case of osteoarticular tuberculosis and tuberculous osteomyelitis of the left foot without pulmonary involvement. Radiol Case Rep 2024;19:6609-13. [Google Scholar] [PubMed]
- 13. Meganathan A, Anu S. A clinical profile of tuberculosis in CKD patients and the response to modified ATT. J Evol Med Dent Sci 2018;30:470-7. [Google Scholar] [PubMed]
- 14. El Bardai G, Kabbali N, Baba H, Chouhani BA, Sqalli Houssaini T. Tuberculosis in dialysis patients in the central region of Morocco: What is the health-care delay? Cureus 2022;14:e30369. [Google Scholar] [PubMed]
- 15. Tangadulrat P, Suwannaphisit S. Tuberculosis septic arthritis of the elbow: A case report and literature review. Cureus 2021;13:e13765. [Google Scholar] [PubMed]
- 16. Gupta S, Parihar A, Singh S, Agarwal A, Agarwal S. Pediatric osteoarticular tuberculosis as a diagnostic dilemma and a review of literature. Cureus 2022;14:e23053. [Google Scholar] [PubMed]
- 17. Held M, Laubscher M, Workman L, Zar HJ, Dunn R. Diagnostic accuracy of GeneXpert MTB/RIF in musculoskeletal tuberculosis: High sensitivity in tissue samples of HIV-infected and HIV-uninfected patients. S Afr Med J 2017;107:854-8. [Google Scholar] [PubMed]
- 18. Dahou H, Younoussa FS, Aragon I, El Aouadi S, El Harras Y, Benaissa E, et al. Primary iliac bone tuberculosis: A case report. Access Microbiol 2025;7:000844.v3. [Google Scholar] [PubMed]
- 19. Kurniawan A, Maruanaya S. Intra operative Ziehl-Neelsen test to establish diagnosis of osteoarticular tuberculosis case: A case report and literature review from multifocal osteoarticular tuberculosis case. Int J Recent Innov Med Clin Res 2024;1:7-15. [Google Scholar] [PubMed]
- 20. Firth G, Lescheid J, Camacho M, Esteves M, Beylis N, Groome M, et al. Extraspinal osteoarticular multidrug-resistant tuberculosis in children: A case series. S Afr Med J 2017;107:983-6. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients March 1, 2026 Tuberculous Synovitis of the Elbow Presenting with Multiple Rice Bodies: A Rare Case Report
March 1, 2026 Tuberculous Synovitis of the Elbow Presenting with Multiple Rice Bodies: A Rare Case Report March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy
March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy