
Patients with pathologic intertrochanteric hip fractures with a background of osteochondroma can be managed via surgical stabilisation as per standard treatment in addition to tumour resection through the most feasible approach based on tumour extension.
Dr Nabil Alassaf, Department of Orthopaedic Surgery, Hail Health Cluster, Hail, Saudi Arabia. E-mail: dr.nabil.alassaf@gmail.com
Abstract
Introduction: Solitary femoral neck osteochondroma (SFNO) usually presents with pain, impingement, or sciatic neuropathy. Concomitant fracture on presentation is rare. This paper describes the treatment approach in such a situation.
Case Report: A 23-year-old male presented after a motor vehicle collision and complained of right hip pain. Clinical assessment and radiological investigations revealed an isolated intertrochanteric femoral fracture adjacent to a posteromedial SFNO. The lesion was resected through a lateral approach, which facilitated simultaneous fracture stabilisation with a cephalomedullary nail. A histological sample confirmed the diagnosis. The fracture healed uneventfully with no recurrence of the lesion.
Conclusion: Asymptomatic posteromedial SFNO presenting with a fracture may respond well to fixation and removal through a lateral approach.
Keywords: Osteochondroma, intertrochanteric fracture, pathologic fracture, cephalomedullary nail.
Osteochondroma is the most common benign bone tumour. In 85% of patients, it presents with a solitary lesion, and in 15% of patients, it manifests as hereditary multiple exostoses (HME). Approximately 50% of osteochondromas are located around the knee. Resection is indicated only for symptomatic compressive lesions or when the adjacent joints are in jeopardy. Malignant transformation and cosmetic factors are infrequent indications for surgical intervention [1]. The overall recurrence rate is about 2%. Interestingly, spontaneous resolution of solitary osteochondromas has been reported [2]. Solitary femoral neck osteochondroma (SFNO) is rare; it requires special attention and careful surgical planning owing to its proximity to neurovascular structures and vulnerable femoral head blood supply and the variety of operative corridors for tumour resection in this area. SFNO may present with pain, neuropathy, limp, limited hip range of motion, and ischiofemoral impingement. Impingement can be exaggerated by the presence of thoracolumbar kyphosis and secondary hip extension [3]. Femoral head osteochondroma likely represents another neoplastic process, namely, Trevor’s disease, which is approached differently [4]. Juxta-articular, extraskeletal osteochondroma has been reported to float in muscles surrounding the femoral neck [5,6]. In this report, we describe a patient with SFNO who presented with an intertrochanteric fracture. We also aimed to review the literature for appropriate treatment methods that may improve decision-making.
A 23-year-old male was brought to the emergency department of our institution after a head-on motor vehicle collision in February 2021. His Glasgow Coma Scale score was 15, with no evidence of haemodynamic instability. His chief complaint was right hip pain and inability to walk. He had been an unbelted front-seat passenger and had been forced under the dashboard, where he felt a snap in his right hip. There were no other injuries. The patient was completely asymptomatic before this presentation and had no medical illness. He underwent surgery for a right proximal humerus fracture that resulted from a high-energy fall 6 years earlier and which had healed uneventfully. An anteroposterior pelvic radiograph at that time was performed as a part of the Advanced Trauma Life Support guidelines, and an asymptomatic right proximal femur lesion, which the patient was not aware of, was noted (Fig. 1).

Figure 1: Pelvic radiograph showing right proximal femur lesion 6 years prior to the current presentation.
On examination, right hip tenderness was detected, and minimal hip range of motion was painful. The motor, sensory, and vascular exams were normal. New radiographs revealed a right hip intertrochanteric fracture in addition to the pre-existing mass (Fig. 2).

Figure 2: Pelvic radiograph obtained in the emergency department revealing right hip intertrochanteric fracture and osteochondroma.
A computed tomography (CT) scan established the diagnosis of SFNO, which was continuous with the displaced fracture (Fig. 3).
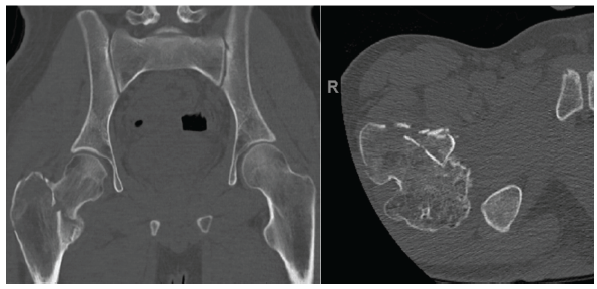
Figure 3: Coronal (left image) and axial (right image) computed tomography views outlining the fracture.
The tumour arose from the femoral neck just proximal to the lesser trochanter, projecting posteromedially. We believe that the priority in this case was to address the fracture and resect as much of the asymptomatic lesion as possible, mainly for histologic diagnosis and better healing. This was achieved in the operating room under general anaesthesia after admission and preparation. To maintain simplicity and ease, we chose the lateral approach in the supine position. The reduction and fixation were aided by a fracture table and a short dual-screw cephalomedullary nail. The tumour was removed in a piecemeal fashion under fluoroscopy. Adequacy of resection was based on clinical and radiographic assessment of the ischiofemoral space. Histopathologic examination confirmed the diagnosis of osteochondroma. The patient was discharged on post-operative day 2 in good condition. He was allowed partial weight bearing for 6 weeks, followed by full weight bearing. At 3 years and 8 months of follow-up (October 2024), the patient reported mild activity-related right lateral thigh pain. However, he demonstrated a full range of motion, had a healed fracture on radiographs, and showed no evidence of recurrence (Fig. 4). We believe that the treatment goals were achieved.
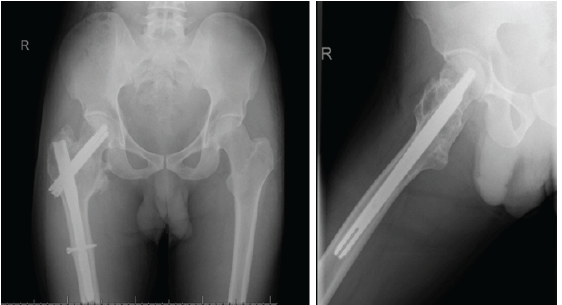
Figure 4: Anteroposterior and lateral follow-up radiographs,
The lateral approach is probably less tedious because it allows for convenient simultaneous reduction and fixation of the fracture with easy intraoperative imaging. However, it does not allow for thorough medial resection. A cephalomedullary nail provides a reliable form of stabilisation but may cause irritation to the iliotibial band. It is probably advantageous to use intramedullary fixation compared to extramedullary plates, especially when the femoral calcar area and the lateral wall are compromised. The tumour in this patient originated from the medial femoral neck. In a study of 100 hips with HME, 79% of proximal femur osteochondromas were found medially [7]. Conservative treatment has been described in patients with minimal symptomatology [8]. After the patient developed complete post-operative sciatic nerve palsy, Jeon et al. warned against approaching a posteriorly protruding tumour through the anterior approach; the patient underwent immediate post-operative exploration, and the nerve recovered 6 months postoperatively [9]. Ghoti et al. excised a posterior femoral neck osteochondroma through a posterior approach in a patient with HME, which resulted in the resolution of symptoms and no recurrence on follow-up after 3 years [10]. Sorel et al. have used surgical hip dislocation to treat femoral neck osteochondroma in 20 hips of HME patients; there was significant improvement in pain and range of motion at the expense of four notable complications: One fibrous nonunion of the trochanteric osteotomy, another osteotomy fixation failure, a pertrochanteric fracture, and avascular necrosis [11]. Small intracapsular lesions are likely amenable to arthroscopic resection. Hip arthroscopy has been used in patients with HME and other hip afflictions such as synovial chondromatosis [12]. Mansor et al. resected a metachondromatosis femoral neck lesion in a child arthroscopically [13]. Alter et al. described arthroscopic hip extended capsulotomy for a 2.2 cm osteochondroma, which was distal to the capsular attachment [14]. Sun et al. used intraoperative CT navigation in 13 patients with femoral neck osteochondroma, 8 of whom were solitary; 9 patients had posterior exposure, whereas four hips were operated on through the anterior approach [15]. We are not aware of any published case of SFNO that presented with a hip fracture. Schubert et al. described posteromedial femoral neck osteochondroma in a 53-year-old woman who was known to have HME. She presented initially with symptoms of ischiofemoral impingement, and 3 months later she was referred with a displaced intracapsular hip fracture that was treated with a total hip replacement [16]. In the series reported by Ramos-Pascua et al., a 66-year-old male patient was noted to have an iatrogenic basicervical femoral neck fracture during excision through an anterior approach of a medial SFNO that was treated by a short cephalomedullary nail [17]. Bottner et al. reported an intraoperative femoral neck fracture during osteochondroma removal in a 44-year-old patient whose osteosynthesis failed and who required total hip arthroplasty [18]. The risk of recurrence after resection of SFNO is low, as there is no single case of recurrence in the relevant papers as summarised in Table 1.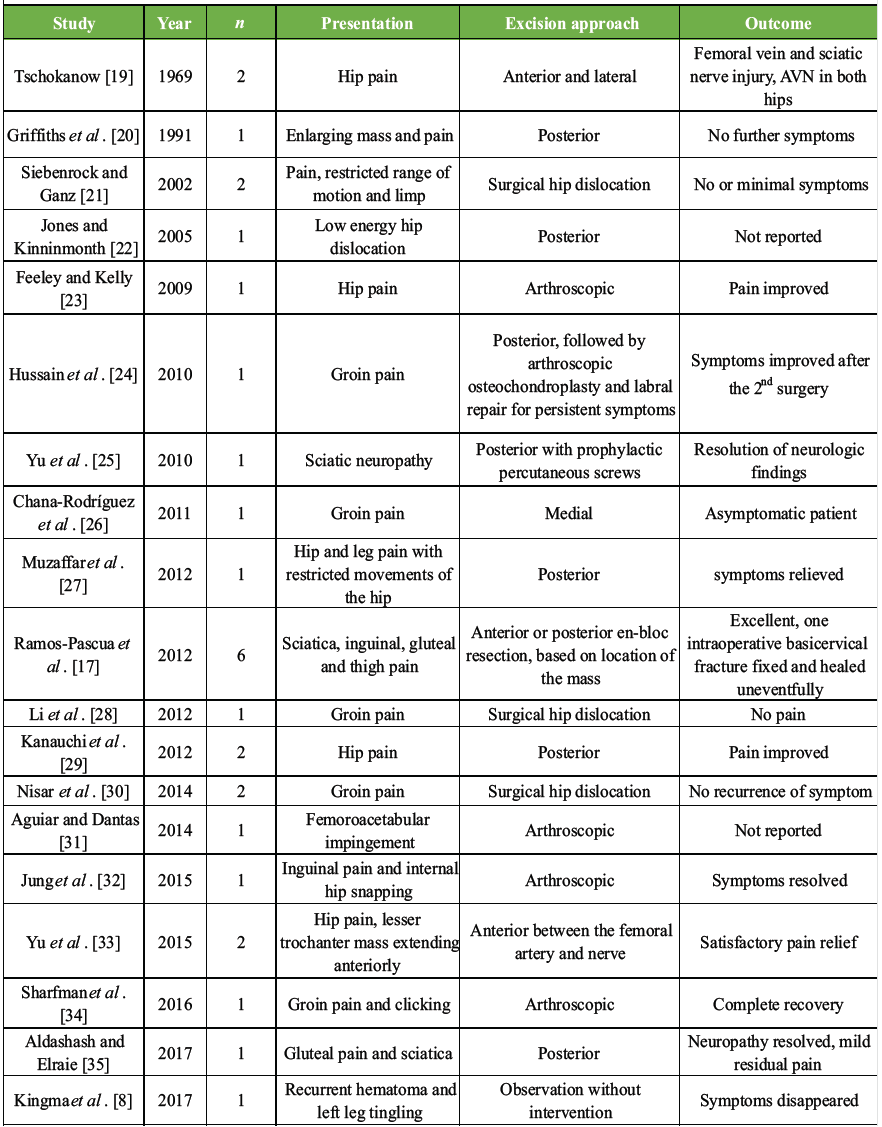
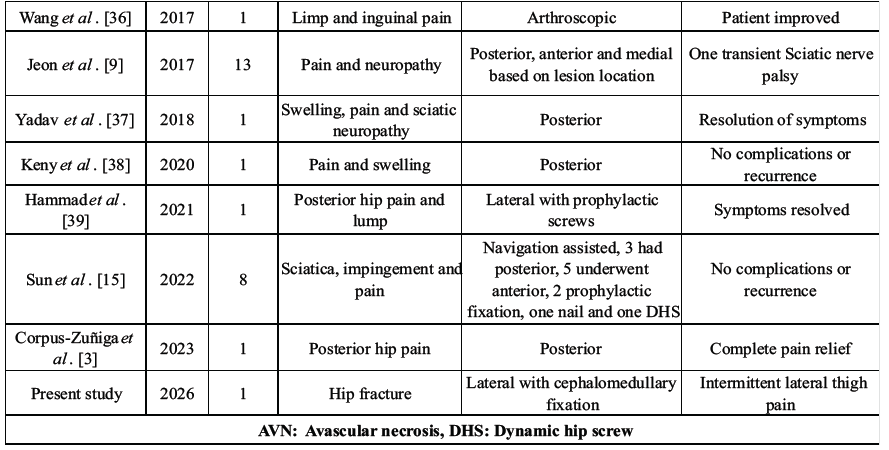
Table 1: Published reports describing solitary femoral neck osteochondroma treatment
The treatment of osteochondroma is based on the presenting symptoms, and the surgical approach is best dictated by the location of the lesion within the femoral neck. Associated actual or impending fractures are fixed through standard techniques and implants.
A lateral approach to surgical fixation and tumour removal can be used to treat extracapsular hip fractures caused by posteromedial SFNO.
References
- 1. Tepelenis K, Papathanakos G, Kitsouli A, Troupis T, Barbouti A, Vlachos K, et al. Osteochondromas: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features and treatment options. In Vivo 2021;35:681-91. [Google Scholar] [PubMed]
- 2. Passanise AM, Mehlman CT, Wall EJ, Dieterle JP. Radiographic evidence of regression of a solitary osteochondroma: A report of 4 cases and a literature review. J Pediatr Orthop 2011;31:312-6. [Google Scholar] [PubMed]
- 3. Corpus-Zuñiga FM, Muramatsu K, Yamashita Y, Mervyn Tec L. Unusual ischiofemoral impingement secondary to osteochondroma in an elderly patient with thoracolumbar kyphosis: A case report. J Orthop Rep 2023;2:100223. [Google Scholar] [PubMed]
- 4. Calafiore F, Fidanza A, Venosa M, Fabiani R, Logroscino G. Hip joint osteochondroma treated with short stem total hip arthroplasty: A case report. Acta Biomed 2023;94:e2023188. [Google Scholar] [PubMed]
- 5. Liu ZJ, Zhao Q, Zhang LJ. Extraskeletal osteochondroma near the hip: A paediatric case. J Pediatr Orthop B 2010;19:524-8. [Google Scholar] [PubMed]
- 6. Kanwat M, Jangira V, Sharma B, Chauhan D. Can an exostosis be free-floating without any continuity to the underlying bone: a diagnostic dilemma? J Clin Orthop Trauma 2017;8:S87-9. [Google Scholar] [PubMed]
- 7. Matsumoto K, Ogawa H, Akiyama H. Radiographic characteristics of the hip joint in skeletally mature patients with multiple hereditary exostoses. Skeletal Radiol 2020;49:1773-9. [Google Scholar] [PubMed]
- 8. Kingma BF, Knobben BA, Somford MP. A motorcyclist with haematomas and tingling in his leg. Ned Tijdschr Geneeskd 2017;161:D633. [Google Scholar] [PubMed]
- 9. Jeon DG, Cho WH, Song WS, Kong CB, Lee SY, Kim DY. The optimal surgical approach and complications in resecting osteochondroma around the lesser trochanter. J Korean Orthop Assoc 2017;52:33-9. [Google Scholar] [PubMed]
- 10. Ghoti S, Mahajan NP, Kondewar P, Pande KP, Chaudhari K. A case report on surgical excision of intracapsular osteochondroma of femur neck using mini-arthrotomy without hip dislocation in a young female with hereditary multiple exostoses. J Orthop Case Rep 2022;12:66-9. [Google Scholar] [PubMed]
- 11. Sorel JC, Façee Schaeffer M, Homan AS, Scholtes VA, Kempen DH, Ham SJ. Surgical hip dislocation according to Ganz for excision of osteochondromas in patients with multiple hereditary exostoses. Bone Joint J 2016;98-B:260-5. [Google Scholar] [PubMed]
- 12. Bonnomet F, Clavert P, Abidine FZ, Gicquel P, Clavert JM, Kempf JF. Hip arthroscopy in hereditary multiple exostoses: A new perspective of treatment. Arthroscopy 2001;17:E40. [Google Scholar] [PubMed]
- 13. Mansor N, Saisu T, Kakizaki J, Oikawa Y, Kamegaya M. Arthroscopic resection of femoral neck osteochondroma: Report of a paediatric case of metachondromatosis. J Orthop Sci 2022;27:739-42. [Google Scholar] [PubMed]
- 14. Alter T, Okoroha KR, Kunze KN, Beck EC, Nho SJ. Arthroscopic femoral osteochondroplasty with capsular plication for osteochondroma of the femoral neck. Arthrosc Tech 2019;8:e1353-9. [Google Scholar] [PubMed]
- 15. Sun Y, Chan CM, Yu F, Li Y, Niu X. Computer navigation-aided excision of proximal femoral osteochondroma: Surgical technique. Comput Math Methods Med 2022;2022:7635945. [Google Scholar] [PubMed]
- 16. Schubert T, Navez M, Galant C, Docquier PL, Acid S, Lecouvet FE. Femoral osteochondroma responsible for ischiofemoral impingement, bursitis, and secondary lipoma arborescens mimicking malignant transformation. Acta Radiol Open 2019;8:1-7. [Google Scholar] [PubMed]
- 17. Ramos-Pascua LR, Sánchez-Herráez S, Alonso-Barrio JA, Alonso-León A. Solitary osteochondromas of the proximal femur. Indication and results of en bloc resection without hip dislocation. Rev Esp Cir Ortop Traumatol 2012;56:24-31. [Google Scholar] [PubMed]
- 18. Bottner F, Rodl R, Kordish I, Winklemann W, Gosheger G, Lindner N. Surgical treatment of symptomatic osteochondroma. A three- to eight-year follow-up study. J Bone Joint Surg Br 2003;85:1161-5. [Google Scholar] [PubMed]
- 19. Tschokanow K. Two cases of osteochondroma of the femur neck. Beitr Orthop Traumatol 1969;16:751-2. [Google Scholar] [PubMed]
- 20. Griffiths HJ, Thompson RC Jr., Galloway HR, Everson LI, Suh JS. Bursitis in association with solitary osteochondromas presenting as mass lesions. Skeletal Radiol 1991;20:513-6. [Google Scholar] [PubMed]
- 21. Siebenrock KA, Ganz R. Osteochondroma of the femoral neck. Clin Orthop Relat Res 2002;394:211-8. [Google Scholar] [PubMed]
- 22. Jones BG, Kinninmonth AW. Low-energy hip dislocation in the young. J Trauma Inj Infect Crit Care 2005;58:638-9. [Google Scholar] [PubMed]
- 23. Feeley BT, Kelly BT. Arthroscopic management of an intraarticular osteochondroma of the hip. Orthop Rev (Pavia) 2009;1:e2. [Google Scholar] [PubMed]
- 24. Hussain W, Avedian R, Terry M, Peabody T. Solitary osteochondroma of the proximal femur and femoral acetabular impingement. Orthopaedics 2010;33:51. [Google Scholar] [PubMed]
- 25. Yu K, Meehan JP, Fritz A, Jamali AA. Osteochondroma of the femoral neck: A rare cause of sciatic nerve compression. Orthopaedics 2010;33:625-6. [Google Scholar] [PubMed]
- 26. Chana-Rodríguez F, López-Capapé D, Rojo-Manaute J, Vaquero-Martín J, Alonso-Martín JM, González-Santander M, et al. Ludloff approach for osteochondroma in the lesser trochanter in a young middle-distance runner. Eur Orthop Traumatol 2011;2:83-5. [Google Scholar] [PubMed]
- 27. Muzaffar N, Bashir N, Baba A, Ahmad A, Ahmad N. Isolated osteochondroma of the femoral neck presenting as hip and leg pain. A case study. Ortop Traumatol Rehabil 2012;14:183-7. [Google Scholar] [PubMed]
- 28. Li M, Luettringhaus T, Walker KR, Cole PA. Operative treatment of femoral neck osteochondroma through a digastric approach in a paediatric patient: A case report and review of the literature. J Pediatr Orthop B 2012;21:230-4. [Google Scholar] [PubMed]
- 29. Kanauchi T, Suganuma J, Kawasaki T, Mochizuki R, Inoue Y, Uchikawa S, et al. Fracture of an osteochondroma of the femoral neck caused by impingement against the ischium. Orthopaedics 2012;35:e1438-41. [Google Scholar] [PubMed]
- 30. Nisar A, Gulhane S, Mahendra A, Meek RM, Patil S. Surgical dislocation of the hip for excision of benign tumours. J Orthop 2014;11:28-36. [Google Scholar] [PubMed]
- 31. Aguiar T, Dantas P. Arthroscopic resection of intra-articular osteochondromas of the hip. Arthrosc Tech 2014;3:e347-50. [Google Scholar] [PubMed]
- 32. Jung HT, Hwang DS, Jeon YS, Kim PS. Arthroscopic resection of osteochondroma of the hip joint associated with internal snapping: A case report. Hip Pelvis 2015;27:43-8. [Google Scholar] [PubMed]
- 33. Yu Y, Sun X, Song X, Tian Z, Zhou Y. A novel surgical approach for the treatment of tumours in the lesser trochanter. Exp Ther Med 2015;10:201-6. [Google Scholar] [PubMed]
- 34. Sharfman ZT, Atzmon R, Gortzak Y, Rotem G, Drexler M, Haviv B, et al. Hip arthroscopy for intra-capsular benign tumours: A case series. J Hip Preserv Surg 2016;3:312-7. [Google Scholar] [PubMed]
- 35. Aldashash F, Elraie M. Solitary osteochondroma of the proximal femur causing sciatic nerve compression. Ann Saudi Med 2017;37:166-9. [Google Scholar] [PubMed]
- 36. Wang SI, Park EH, Yoon SJ, Kim JR. Intra-articular osteochondroma of the posteroinferior femoral neck associated with hip joint osteochondromatosis: A case report. Mol Clin Oncol 2017;7:915-8. [Google Scholar] [PubMed]
- 37. Yadav S, Maurya P, Kumar M, Arya R. Osteochondroma of the posterior femoral neck: A rare cause of sciatic nerve compression. Global J Res Anal 2018;7:48-9. [Google Scholar] [PubMed]
- 38. Keny S, Dahapute A, Shah S, Marathe N. Surgical excision of a solitary osteochondroma arising from the lesser trochanter in an adult: A case report. Int J Res Orthop 2020;6:1112-6. [Google Scholar] [PubMed]
- 39. Hammad Y, Saleh HA, Aburumman IF, Balasim M, Al-Hyari MI, Al-Ajlouni J. A rare case of intra-articular osteochondroma of the femoral neck: A case report. J Ortho Case Rep 2021;11:91-6. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 “The Wayward Screw”: A Rare Case Report of Intrapelvic Migration of a Cephalomedullary Lag Screw
November 1, 2025 “The Wayward Screw”: A Rare Case Report of Intrapelvic Migration of a Cephalomedullary Lag Screw July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis