
Isolated trochlear fractures are rare injuries that require CT evaluation and stable anatomical fixation for optimal functional recovery.
Dr Mahammad Suhail, Jawahar Lal Nehru Medical College, Ajmer, Rajasthan, India. E-mail: mahammadsuhailputtur@gmail.com
Abstract
Introduction: Isolated fractures of the humeral trochlea are exceedingly rare because of the trochlea’s deep intra-articular position and anatomical protection from direct trauma. The articular notch formed by the olecranon and coronoid processes shields the trochlea, which also lacks direct muscular or ligamentous attachments. Such fractures typically occur in conjunction with injuries involving the capitellum or the medial and lateral condyles.
Case Report: We report the case of a 35-year-old male who sustained an isolated trochlear fracture following a physical assault. Initial anteroposterior radiographs demonstrated irregularity of the medial joint space, while the lateral view revealed an intra-articular, half-moon-shaped fragment displaced anterosuperiorly. Computed tomography (CT) confirmed the isolated trochlear fracture. The patient underwent open reduction and internal fixation through a medial approach. At 12 months postoperatively, the patient achieved a complete functional recovery with Mayo Elbow Performance Index score of 100.
Discussion: Isolated trochlear fractures in adults are uncommon and are frequently associated with capitellar fractures or elbow dislocations. Radiographs and CT scans are essential diagnostic tools, with CT remaining the gold standard for definitive diagnosis and preoperative planning. Stable anatomical fixation through a medial approach provides excellent functional outcomes while minimizing complications.
Conclusion: Isolated trochlear fractures are exceptionally rare injuries. Early diagnosis with CT imaging and stable internal fixation through a medial approach can provide excellent functional and radiological outcomes.
Keywords: Trochlear fracture, distal humerus, coronal shear fracture, Herbert screw, elbow trauma, open reduction, internal fixation.
Isolated fractures of the humeral trochlea are extremely rare injuries and were first described by Laugier in 1853. Despite advances in the understanding and treatment of distal humeral fractures, the exact mechanism responsible for isolated trochlear fractures remains unclear. The Orthopaedic Trauma Association classifies these injuries as type 13-B3, although this classification is infrequently used in clinical practice. The rarity of isolated trochlear fractures is attributed to the trochlea’s deep intra-articular position, its protection by the olecranon and coronoid processes, and the absence of direct muscular or ligamentous attachments. Most trochlear fractures occur in association with capitellar fractures, condylar injuries, elbow dislocations, or ligamentous disruptions. Treatment options include fragment excision or open reduction and internal fixation (ORIF). We present a rare case of an isolated displaced trochlear fracture managed successfully through a medial approach using Herbert screw fixation, resulting in excellent functional recovery.
A 35-year-old male sustained a physical assault to the left elbow while it was in extension and supination. Clinical evaluation revealed pain and swelling localised to the medial aspect of the elbow, with restricted flexion and extension, while pronation and supination were preserved [1]. Anteroposterior radiographs showed irregularity of the medial joint space, while the lateral view demonstrated an intra-articular, half-moon–shaped fragment displaced anterosuperiorly, initially suggestive of a capitellar fracture (Fig. 1).

Figure 1: Anteroposterior and lateral radiographs of the left elbow demonstrating an intra-articular coronal shear fracture of the trochlea with anterior displacement of the fragment.
Computed tomography (CT) confirmed an isolated coronal shear fracture of the trochlea without capitellar involvement (Fig. 2).
Figure 2: Three-dimensional computed tomography reconstruction showing an isolated fracture of the humeral trochlea without associated capitellar involvement.
The patient underwent ORIF through a medial approach, between the triceps posteriorly and brachialis anteriorly (Fig. 3).
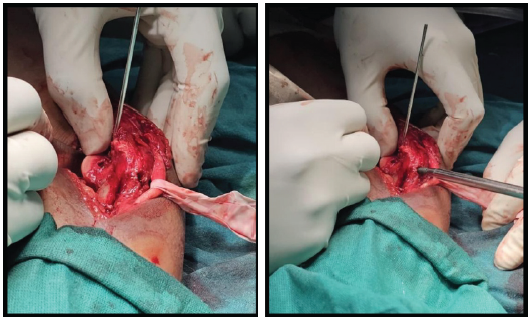
Figure 3: Intraoperative image showing exposure through the medial approach between the brachialis anteriorly and triceps posteriorly.
The ulnar nerve was carefully identified and protected. Exposure of the joint capsule required partial disinsertion of the humeral origin of the pronator teres, preserving the intact medial collateral ligament [2]. Intraoperatively, the trochlear fragment was displaced upward and forward, with an intact posterior wall. The articular cartilage appeared macroscopically intact without visible chondral defects; however, no quantitative cartilage assessment system was utilised. Reduction was facilitated by elbow flexion, allowing adequate retraction of the brachialis muscle [3]. Fixation was achieved using one 3.5-mm Herbert screw and one partially threaded 4.5-mm cancellous screw inserted from the non-articular surface [4]. Both screws were directed obliquely from posterior to anterior and medial to lateral, securing the trochlea to the capitellum (Figs. 4 and 5).
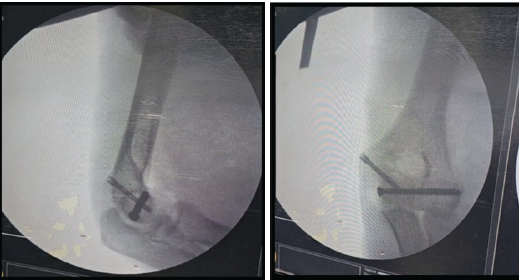
Figure 4: Intraoperative anteroposterior and lateral radiographs demonstrating fixation with Herbert screw and cancellous screw.
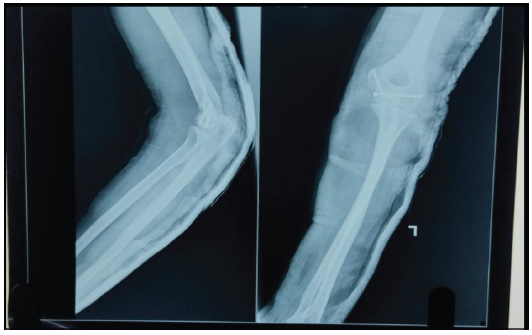
Figure 5: Post-operative lateral and anteroposterior radiographs demonstrating fixation with Herbert screw and cancellous screw.
The ulnar nerve was reassessed to rule out compression, and the elbow demonstrated satisfactory motion in both flexion-extension and pronation-supination planes. The wound was closed in layers, and a posterior plaster slab was applied with the elbow maintained at 90° flexion.
Outcome and follow-up:
At 3 months postoperatively, the patient exhibited pain-free motion from 0° to 135° of flexion, with no evidence of instability (Fig. 6).

Figure 6: Clinical photograph at 3 months follow-up showing restored elbow flexion and extension.
Follow-up radiographs confirmed maintained reduction and complete fracture union without any signs of avascular necrosis or degenerative changes (Fig. 7).
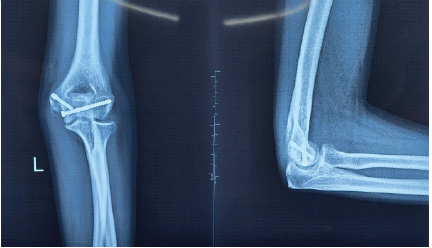
Figure 7: Radiographic outcome at one year follow-up
At 12 months, the patient achieved full functional recovery, attained a Mayo Elbow Performance Index score of 100, and successfully resumed all pre-injury activities.
The humeral trochlea is an essential component of the elbow joint, facilitating smooth ulnohumeral articulation. Its disruption can lead to instability and stiffness if inadequately treated. Isolated trochlear fractures are uncommon due to the trochlea’s deep intra-articular position and absence of direct soft-tissue attachments. The exact biomechanical mechanism responsible for isolated trochlear fractures remains uncertain. Proposed mechanisms include axial loading transmitted through the ulna during elbow extension or varus stress resulting in coronal shear forces across the trochlea. In the present case, the mechanism is inferred from the injury history but was not experimentally investigated. Consistent with our findings, Rehman et al. (2025) reported a successful case of open reduction and Herbert screw fixation via a medial approach, emphasising the importance of precise anatomical reduction for optimal functional recovery [5]. Similarly, Gonçalves and Ring (2016) demonstrated that the medial approach preserves vascularity and minimises the risk of avascular necrosis, supporting our chosen surgical exposure [6]. Studies by Yu et al. highlighted the efficacy of Herbert screw fixation in coronal shear fractures of the capitellum, achieving excellent articular congruity and motion restoration—outcomes comparable to ours [7,8]. The mechanism of injury in our patient, involving axial loading through an outstretched hand, aligns with their proposed biomechanical explanations [9]. Our result of complete motion recovery further supports the consensus that stable fixation and anatomical reduction are key to preventing post-traumatic arthritis [10,11]. CT remains the diagnostic gold standard, as also recommended by these authors. Hence, our case reinforces the growing evidence supporting ORIF via a medial approach using Herbert screws as an effective strategy for achieving optimal functional outcomes. Although conservative treatment has been described for minimally displaced trochlear fractures, displaced intra-articular fractures generally require anatomical reduction and stable fixation to restore joint congruity and permit early mobilisation. Our case involved a displaced coronal shear fracture and was therefore managed surgically. The present case adds to the limited literature on isolated humeral trochlear fractures and highlights the importance of maintaining a high index of suspicion in patients presenting with medial elbow pain following trauma. Unlike most previously reported cases, our patient had no associated capitellar fracture, elbow dislocation, or ligamentous instability. Furthermore, successful management through a medial approach using combined Herbert screw and cancellous screw fixation resulted in excellent functional recovery without complications. This case reinforces the role of early CT-based diagnosis and stable anatomical fixation in achieving favourable clinical outcomes. No evidence of hardware prominence, screw penetration, heterotopic ossification, ulnar nerve symptoms, infection, loss of fixation, or avascular necrosis was observed during the 12-month follow-up period [Table 1].
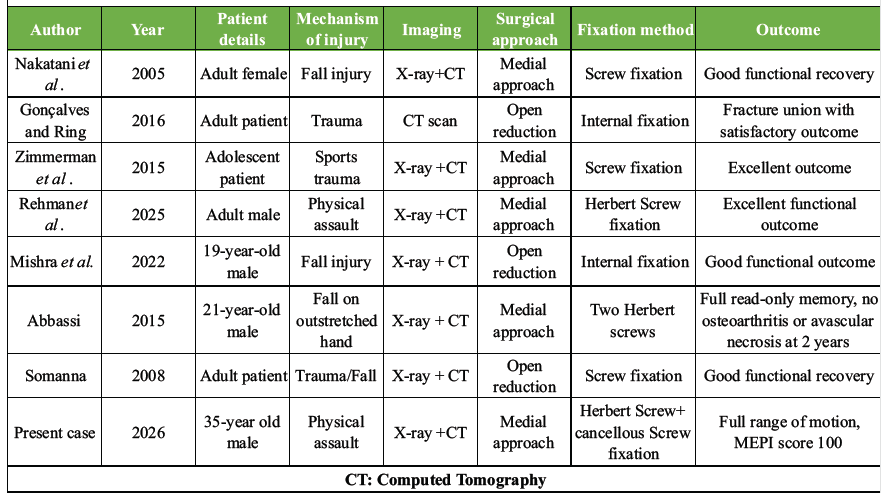
Table 1: Evidence summary of previously reported isolated trochlear fractures.
Limitations:
This report describes a single patient, and therefore, the findings cannot be generalised to all isolated trochlear fractures. The rarity of this injury limits the availability of larger comparative studies and standardised treatment protocols. Magnetic resonance imaging (MRI) was not performed because there were no clinical signs of ligamentous instability, and CT adequately characterised the fracture pattern for surgical planning. Functional assessment was primarily based on the Mayo Elbow Performance Index, and additional patient-reported outcome measures, such as Disabilities of the Arm, Shoulder, and Hand or Oxford Elbow Score, were not available. Long-term follow-up beyond twelve months would be valuable to assess post-traumatic arthritis, avascular necrosis, and late stiffness. Post-operative CT or MRI was not obtained because radiographs demonstrated satisfactory union and restoration of elbow function.
Isolated trochlear fractures are rare injuries that demand a high index of suspicion for diagnosis. Detailed CT is essential for accurate fracture characterisation and surgical planning. Open reduction and stable internal fixation through a medial approach can achieve excellent functional recovery, restore elbow stability, and minimise the risk of post-traumatic stiffness or degenerative arthritis.
Isolated humeral trochlea fractures are rare; CT aids diagnosis, and stable ORIF provides excellent functional outcomes.
References
- 1. Abdoli A, Farhoud AR, Kamrani RS. Treatment of distal humerus articular fracture with pin-and-plate technique. J Hand Surg Asian Pac Vol 2020;25:332-9. [Google Scholar] [PubMed]
- 2. Watson JJ, Bellringer S, Phadnis J. Coronal shear fractures of the distal humerus: Current concepts and surgical techniques. Shoulder Elbow 2020;12:124-35. [Google Scholar] [PubMed]
- 3. Carroll MJ, Athwal GS, King GJ, Faber KJ. Capitellar and trochlear fractures. Hand Clin 2015;31:615-30. [Google Scholar] [PubMed]
- 4. Zimmerman LJ, Jauregui JJ, Aarons CE. Isolated shear fracture of the humeral trochlea in an adolescent: A case report and literature review. J Pediatr Orthop B 2015;24:412-7. [Google Scholar] [PubMed]
- 5. Rehman A, Nasrumminallah M, Rehan F, Kumar H, Ashfaq A, Teena FN. Surgical management of an isolated humeral trochlear fracture: A rare case report and literature review. Int J Surg Case Rep 2025;129:111147. [Google Scholar] [PubMed]
- 6. Gonçalves LB, Ring DC. Fractures of the humeral trochlea: Case presentations and review. J Shoulder Elbow Surg 2016;25:e151-5. [Google Scholar] [PubMed]
- 7. Chamseddine A, Hamdan H, Obeid B, Zein H. Articular coronal fractures of the distal humerus. Chir Main 2009;28:352-62. [Google Scholar] [PubMed]
- 8. Yu T, Tao H, Xu F, Hu Y, Zhang C, Zhou G. Management of isolated coronal shear fractures of the humeral capitellum with Herbert screw fixation through an anterolateral approach. BMC Musculoskelet Disord 2018;19:108. [Google Scholar] [PubMed]
- 9. Yu T, Tao H, Xu F, Hu Y, Zhang C, Zhou G. Comparison of lateral approach versus anterolateral approach with Herbert screw fixation for isolated coronal shear fractures of humeral capitellum. J Orthop Surg Res 2019;14:230. [Google Scholar] [PubMed]
- 10. Nauth A, McKee MD, Ristevski B, Hall J, Schemitsch EH. Distal humeral fractures in adults. J Bone Joint Surg Am 2011;93:686-700. [Google Scholar] [PubMed]
- 11. Nakatani T, Sawamura S, Sakurai A, Imaizumi Y, Fujioka H, Tomioka M, et al. Isolated fracture of the trochlea: A case report. J Shoulder Elbow Surg 2005;14:340-3. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report
February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature
September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature May 1, 2026 Temporary Fusionless Occipitocervical Fixation of Bilateral Occipital Condylar Avulsion Fractures in an Adult
May 1, 2026 Temporary Fusionless Occipitocervical Fixation of Bilateral Occipital Condylar Avulsion Fractures in an Adult May 1, 2026 Medial Hoffa’s Fracture Treated with Subvastus Approach – Case Series
May 1, 2026 Medial Hoffa’s Fracture Treated with Subvastus Approach – Case Series