
Biological viability, rather than radiographic bone appearance alone, should guide surgical decision-making, as fixation may fail in biologically compromised distal femoral fractures and salvage reconstruction may be required.
Hirokazu Takai, MD, Department of Orthopaedic Surgery, Kumamoto Kinoh Hospital, 6-8-1 Yamamuro, Kita-Ku, Kumamoto, 860-8518 Japan. Tel: +81-96-345-8111. E-mail: hirokazoid@hotmail.co.jp
Abstract
Introduction: Supracondylar femoral refracture in the setting of post-traumatic osteoarthritis presents a complex reconstructive challenge, particularly when prior fracture healing is incomplete and knee function is severely compromised. In such cases, conventional fixation or standard total knee arthroplasty may be associated with a high risk of failure and poor functional recovery.
Case Report: A 77-year-old man with a remote history of distal femoral fracture, including a Hoffa fracture, presented with chronic pain, severe stiffness, and marked functional limitation. Following a fall, he sustained a supracondylar refracture. Radiographs and pre-operative computed tomography demonstrated advanced post-traumatic osteoarthritis, partial non-union, dense sclerosis, loss of normal cancellous architecture, and chronic distal femoral deformity. Despite apparently preserved bone stock on plain radiographs, these findings suggested poor biological healing potential. Intraoperatively, minimal bleeding from the distal femoral bone further supported severe biological compromise. Given the high risk of failed union with further internal fixation, persistent non-union, and poor functional recovery, one-stage distal femoral replacement using a megaprosthesis was performed. The patient achieved uneventful recovery with improved pain, range of motion, and ambulation.
Conclusion: Megaprosthetic reconstruction represents a rational salvage option for supracondylar femoral refracture in biologically compromised post-traumatic knees. Surgical decision-making should prioritize biological viability and realistic functional restoration rather than radiographic bone appearance alone.
Keywords: Supracondylar femur fracture, refracture, non-union, post-traumatic osteoarthritis, megaprosthesis, total knee arthroplasty.
Supracondylar femoral fractures in the setting of post-traumatic osteoarthritis present a complex reconstructive challenge, particularly when prior healing is incomplete and knee function is severely compromised. Conventional treatment options, including open reduction and internal fixation or total knee arthroplasty (TKA), may be associated with suboptimal outcomes in cases with non-union or compromised biological viability [1,2]. Although megaprosthetic reconstruction has been widely used in oncologic settings, its role in non-tumor conditions, such as complex distal femoral fractures, has expanded in recent years and is increasingly being adopted [3,4,5].
A 77-year-old man presented with worsening left knee pain and inability to ambulate following a fall. He had a remote history of distal femoral fracture, including a Hoffa fracture, treated surgically approximately 40 years earlier. Since then, he had experienced chronic pain, severe stiffness, and progressive functional limitation of the knee. On examination, the knee showed marked restriction of motion with significant pain. Pre-injury radiographs demonstrated advanced post-traumatic osteoarthritis with sclerotic changes in the distal femur, suggesting chronic structural abnormality even before the present injury (Fig. 1). Following the recent trauma, radiographs revealed a supracondylar femoral refracture. Notably, despite sustaining an acute fracture, the affected knee showed minimal swelling and absence of subcutaneous hemorrhage on clinical examination, suggesting an unexpectedly limited soft-tissue response for an acute fracture (Fig. 2). Preoperative computed tomography (CT) with multiplanar reconstruction demonstrated chronic structural abnormalities of the distal femur, including dense abnormal sclerosis, partial non-union of the previous Hoffa fracture, loss of normal cancellous architecture, and post-traumatic deformity, suggesting poor biological healing potential (Fig. 3). Although bone stock appeared preserved on plain radiographs, these findings suggested that further internal fixation would carry a high risk of failed union because of the compromised biological environment, particularly in the setting of severe pre-existing functional impairment. Therefore, a one-stage megaprosthetic TKA was selected. Intraoperatively, the distal femoral bone showed minimal bleeding despite adequate exposure, and the fracture surfaces appeared sclerotic, consistent with impaired biological viability (Fig. 4). A distal femoral megaprosthesis was implanted with satisfactory alignment (Fig. 5). Post-operatively, the patient had an uneventful recovery. At 1-year follow-up, the patient achieved significant pain relief and functional recovery, with a range of motion of 0–110° and independent ambulation. Post-operative radiographs showed satisfactory implant alignment without evidence of periprosthetic fracture or implant loosening.
Distal femoral refracture associated with post-traumatic osteoarthritis represents a complex condition that extends beyond a simple fracture, as it may occur in the setting of pre-existing non-union and a compromised biological environment. Therefore, appropriate surgical decision-making is critically important. In the present case, refracture occurred in the setting of sclerotic bone and partial non-union resulting from a previous fracture, representing a pathology distinct from typical traumatic fractures. Internal fixation is generally considered the standard treatment for distal femoral fractures; however, successful bone healing requires not only mechanical stability but also adequate biological factors, including sufficient blood supply and cellular activity. In cases complicated by refracture or pre-existing non-union, poor biological conditions are known to increase the risk of fixation failure and delayed union [1,2]. In elderly patients with distal femoral non-union, repeated fixation may be particularly prone to failure because of poor bone stock, metaphyseal bone loss, prior surgeries, and limited ability to comply with protected weight-bearing [1]. In this case, despite the acute fracture, the combination of an unexpectedly limited soft-tissue response, preoperative CT findings showing dense structural abnormalities with loss of normal cancellous architecture, and almost no intraoperative bleeding collectively suggested markedly reduced biological viability. Thus, although bone stock appeared preserved radiographically, the bone was biologically compromised. Under such conditions, repeated attempts at internal fixation may lead to treatment delay or failure. The non-union scoring system (NUSS) has been proposed as a framework for guiding treatment strategies in non-union by integrating factors related to bone condition, soft tissue status, and patient-related variables [6,7]. More recent clinical discussion has continued to support its usefulness in stratifying non-union severity and identifying patients who may require salvage procedures rather than repeated fixation [8]. In the present case, the presence of non-union, dense and structurally abnormal sclerotic bone, minimal intraoperative bleeding, and pre-existing biological compromise suggested a biologically unfavorable environment in which salvage procedures—including arthrodesis or prosthetic reconstruction—may be more appropriate than further osteosynthesis [2,6,7,8]. While NUSS provides a useful framework for assessing non-union severity, the actual biological viability of the bone remains critical in determining whether fixation is realistically feasible. In recent years, the use of megaprostheses for distal femoral reconstruction has expanded beyond oncologic indications to include complex fractures, non-union, and refracture in non-neoplastic conditions [3,4,5]. Registry data have also shown an apparent shift in megaprosthesis use toward trauma-related indications, supporting this broader contemporary role [5]. Particularly in elderly patients or those with biologically compromised bone, megaprosthetic reconstruction allows immediate full weight-bearing, facilitates early rehabilitation, and promotes rapid functional recovery, including activities of daily living [1,4,9]. However, complication rates remain substantial. Recent reviews and retrospective series have shown that megaprosthetic reconstruction is associated with high complication rates, often in the range of approximately 30–50%, with infection representing one of the most important causes of failure [3,9,10]. This risk profile should be weighed carefully against the expected difficulty of fracture healing in biologically compromised cases. Regarding implant longevity, survivorship in non-oncologic salvage cases has been reported to be acceptable at mid-term follow-up. A recent review suggested approximately 80% survivorship at 5 years in non-oncologic settings, although longer-term durability remains variable and may decline over time [3]. In a salvage arthroplasty series using resection prostheses, revision-free implant survivorship was reported as 92% at both 5 and 10 years, indicating that durable outcomes are achievable in selected cases [11]. Similarly, satisfactory medium-term clinical outcomes have been reported after distal femoral replacement for acute comminuted periprosthetic fractures [12]. In contrast, long-term oncologic data demonstrate the cumulative burden of failure over time, with reoperation rates of 22.6% at 5 years, 30.1% at 10 years, and 42.5% at 20 years, underscoring the persistent long-term risk associated with these implants [13]. Nevertheless, despite these risks, megaprosthetic reconstruction remains a reasonable option in cases where bone healing is unlikely, as it enables early functional recovery. In the present case, internal fixation was deemed unlikely to achieve union, and a one-stage megaprosthetic TKA was selected, resulting in effective pain relief and favorable functional outcomes. From a decision-making perspective, comparative studies evaluating distal femoral replacement versus internal fixation for periprosthetic distal femoral fractures have not consistently shown major differences in mortality or overall complication rates; however, distal femoral replacement may offer practical advantages in early weight-bearing and faster functional recovery, particularly in elderly or frail patients [9,14,15]. Therefore, treatment selection should not be based solely on the theoretical preservation of bone stock but also on whether fixation is biologically and functionally realistic in the individual patient. Although megaprosthetic reconstruction carries risks, such as infection and mechanical complications, and demonstrates a different outcome profile compared with primary TKA, careful patient selection is essential. This is a single case report, and long-term follow-up is necessary; however, in cases of refracture with a biologically compromised bone environment, our findings suggest that initial salvage surgery may be more appropriate than repeated fixation attempts.
Supracondylar femoral refractures in post-traumatic osteoarthritic knees with impaired biological viability present a significant reconstructive challenge. Even when radiographic bone stock appears preserved, conventional fixation may fail if biological healing potential is severely compromised. In such cases, megaprosthetic TKA may represent a rational and effective salvage option for pain relief and functional recovery.
Preserved radiographic bone stock does not guarantee adequate healing potential. When biological viability is compromised, fixation may fail, and salvage reconstruction may be a more appropriate strategy for restoring function and relieving pain.
References
- 1. RajasekaranRB, PalanisamiDR, NatesanR, JayaramarajuD, RajasekaranS. Megaprosthesis in distal femur nonunions in elderly patients-experience from twenty four cases.Int Orthop2020;44:677-84. [Google Scholar] [PubMed]
- 2. KarBK, OjhaMM, YadavSK, AgrawalAC, KowshikS. Distal femur tumor megaprosthesis for non-union of supracondylar femur fracture after failed osteosynthesis. An ingenious solution. J Orthop Case Rep 2021;11:16-9. [Google Scholar] [PubMed]
- 3. Dumaine, V. Complications of distal femur megaprostheses. Orthop Traumatol Surg Res 2026;112: [Google Scholar] [PubMed]
- 4. MeluzioMC, OlivaMS, MinutilloF, ZiranuA, SaccomannoMF, MaccauroG. The use of knee mega-prosthesis for the management of distal femoral fractures: A systematic review. Injury2020;51 Suppl 3:S17-22. [Google Scholar] [PubMed]
- 5. Puttock DR, Howard DP, Eastley NC, Ashford RU. Apparent trends in the use of femoral megaprostheses: An analysis from the National Joint Registry. Arthroplasty2022;4: [Google Scholar] [PubMed]
- 6. CaloriGM, PhillipsM, JeetleS, TagliabueL, GiannoudisPV. Classification of non-union: Need for a new scoring system? Injury2008;39 Suppl 2:S59-63. [Google Scholar] [PubMed]
- 7. CaloriGM, ColomboM, MazzaEL, MazzolaS, MalagoliE, MarelliN, et al. Validation of the non-union scoring system in 300 long bone non-unions. Injury 2014;45 Suppl 6:S93-7. [Google Scholar] [PubMed]
- 8. GaddiD, GattiSD, PiattiM, PoliA, DeRosa L, RigantiA, et al. Non-union scoring system (NUSS): Is it enough in clinical practice? Indian J Orthop 2023;57:137-45. [Google Scholar] [PubMed]
- 9. DeMarco D, MessinaF, MeschiniC, OlivaMS, RovereG, MaccagnanoG, et al. Periprosthetic knee fractures in an elderly population: open reduction and internal fixation vs distal femur megaprostheses. Orthop Rev (Pavia) 2022;14: [Google Scholar] [PubMed]
- 10. SukhonthamarnK, StronyJT, PatelUJ, BrownSA, NazarianDG, ParviziJ, et al. Distal femoral replacement and periprosthetic joint infection after non-oncological reconstruction: A retrospective analysis. J Arthroplasty 2021;36:3959-65. [Google Scholar] [PubMed]
- 11. MolenaersB, ArnoutN, BellemansJ. Complex total knee arthroplasty using resection prostheses at mid-term follow-up. Knee2012;19:550-4. [Google Scholar] [PubMed]
- 12. MatarHE, BlochBV, JamesPJ. Distal femoral replacements for acute comminuted periprosthetic knee fractures: Satisfactory clinical outcomes at medium-term follow-up. Arthroplast Today2021;7:37-42. [Google Scholar] [PubMed]
- 13. OguraK, YakoubMA, BolandPJ, HealeyJH. Finn/orthopaedic salvage system distal femoral rotating-hinge megaprostheses in oncologic patients: Long-term complications, reoperations, and amputations. J Bone Joint Surg Am 2021;103:705-14. [Google Scholar] [PubMed]
- 14. Darrith B, Bohl DD, Karadsheh MS, Sporer SM, Berger RA, Levine BR. Periprosthetic fractures of the distal femur: Is open reduction and internal fixation or distal femoral replacement superior? J Arthroplasty 2020;35:1402-6. [Google Scholar] [PubMed]
- 15. HoellwarthJS, FourmanMS, CrossettL, GoodmanM, SiskaP, MoloneyGB, et al. Equivalent mortality and complication rates following periprosthetic distal femur fractures managed with either lateral locked plating or a distal femoral replacement. Injury 2018;49:392-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Non-union Hoffa’s fracture in an Adult Male managed with Total Knee Arthroplasty : A Rare Case Report
September 1, 2025 Non-union Hoffa’s fracture in an Adult Male managed with Total Knee Arthroplasty : A Rare Case Report September 10, 2021 Distal Femur Tumor Megaprosthesis for Non-union of Supracondylar Femur Fracture after Failed Osteosynthesis. An Ingenious Solution.
September 10, 2021 Distal Femur Tumor Megaprosthesis for Non-union of Supracondylar Femur Fracture after Failed Osteosynthesis. An Ingenious Solution. July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report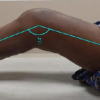 July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes