
Unstable distal-third femoral shaft fractures do not always require poller screws or cerclage. With careful limb positioning and controlled indirect reduction, alignment can be achieved and maintained during retrograde nailing.
Dr Jeff Walter Rajadurai OR, Department of Orthopaedics, Madha Medical College and Research Institute, Chennai, Tamil Nadu, India. E-mail: jeffy.walter@gmail.com
Abstract
Introduction: Distal-third femoral shaft fractures in the elderly are rarely straightforward. Reduction and fixation are challenging due to poor bone quality, an unstable fracture pattern, and not enough room to work. Retrograde nailing is an accepted solution, but in long-oblique fractures, maintaining alignment is often the real problem. Many surgeons depend on poller screws, cerclage wires, or temporary plates to hold the reduction. In this report, we describe a case where none of these were used. The fracture was reduced and held using indirect methods alone.
Case Report: A 72-year-old female presented after a low-energy fall with a long-oblique fracture in the distal third of the femoral shaft. The bone was clearly osteoporotic, and the fracture was unstable by nature. Under image guidance, reduction was achieved using traction, rotation, and careful limb positioning. The fracture site was not opened. No poller screws, cerclage wires, joysticks, or temporary plates were used. Once alignment was satisfactory, a retrograde nail was inserted. The reduction remained stable during guidewire passage and reaming. Postoperatively, alignment was maintained. Callus formation was seen progressively, and the fracture united by 5 months.
Discussion: Most reports on distal-third femoral fractures treated with retrograde nails describe the use of some form of mechanical assistance to control reduction, especially in osteoporotic bone or long-oblique patterns. The concern is always the same – loss of alignment during reaming. In this case, reduction was maintained by paying close attention to limb position, soft-tissue tension, and fluoroscopic control. No adjuncts were required. This challenges the routine instinct to add hardware for control and highlights the value of respecting soft-tissue-guided reduction, even in fractures that appear unstable on imaging.
Conclusion: Even in an osteoporotic, long-oblique distal-third femoral shaft fracture, stable alignment can be achieved without additional reduction tools. When indirect reduction principles are applied patiently and monitored carefully, retrograde nailing remains a reliable option.
Keywords: Retrograde nailing, osteoporosis, distal femur, collar screw, long-oblique fracture.
Distal-third femoral shaft fractures in elderly patients are rarely simple. The combination of weak bones, unstable fracture type, and a small operating space makes both reduction and fixation hard. Locking plates have traditionally been used in this region, but retrograde intramedullary nailing is now increasingly favored because of its biomechanical advantages and the fact that it avoids extensive soft-tissue stripping, which is particularly relevant in osteoporotic femora [1,2,3]. The real difficulty, however, lies in controlling alignment in the distal segment. Short metaphyseal fragments, long-oblique patterns, and poor bone stock often lead surgeons to add cerclage wires, poller screws, or even temporary plates to hold the reduction [4,5,6,7].
The idea of indirect reduction is not new. Maniscalco and Regazzoni had already highlighted the importance of the soft-tissue envelope in guiding fragments into alignment without direct exposure [1,5]. Despite this, in day-to-day practice, many surgeons still depend on mechanical adjuncts for distal-third fractures because reduction tends to drift during reaming or nail passage [8,9,10]. This report describes an unstable distal-third long-oblique femoral shaft fracture in an elderly osteoporotic woman, treated with a retrograde nail using pure indirect reduction alone, without poller screws, cerclage, clamps, or temporary plating. The case shows that with careful control of traction, rotation, and fluoroscopy, a stable axis can still be achieved in a pattern where most would instinctively reach for additional tools.
A 72-year-old female presented after a low-energy fall at home with severe pain in the right thigh and inability to bear weight. Radiographs showed a comminuted long-oblique fracture in the distal third of the femoral shaft. The distal fragment was short, osteoporotic, and mildly translated. There was no intra-articular extension (Fig. 1).

Figure 1: Pre-operative X-ray showing long-oblique fracture in the distal third of the femoral shaft.
Considering her age and bone quality, retrograde intramedullary nailing was chosen. This decision was supported by existing evidence favoring close-canal alignment, minimal soft-tissue disruption, and acceptable outcomes in similar osteoporotic fracture patterns [1,3,5].
Under spinal anesthesia, she was positioned supine on a radiolucent table. Traction was applied through the ankle and allowed to settle naturally. The fracture was not exposed. Reduction was achieved using traction-induced ligamentotaxis, gentle internal and external rotation through the foot, slight adduction to counter the varus tendency, and controlled manipulation of the thigh under fluoroscopy. The aim was to let the limb find its own alignment rather than force it. No reduction clamps, joysticks, cerclage wires, poller screws, or temporary plates were used at any point.
Once alignment appeared satisfactory, the entry point was made through the intercondylar notch, and guidewire insertion was begun. As expected in osteoporotic metaphyseal bone, the wire showed a tendency to drift, but this was controlled with sustained traction and constant fluoroscopic monitoring. Reaming was performed carefully and deliberately, avoiding over-reaming that could destabilize the reduction, a problem highlighted by several authors in distal-third fractures [7,9,11,12] (Fig. 2 and 3).
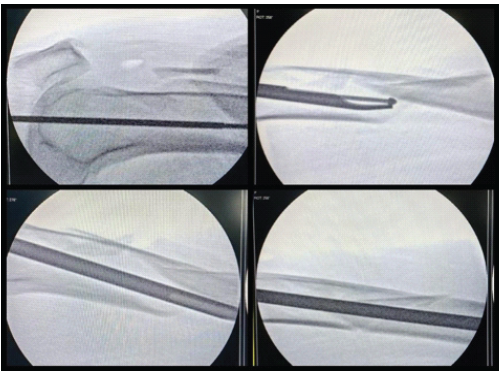
Figure 2: Intra op images showing guidewire entry and reduction maneuvers.
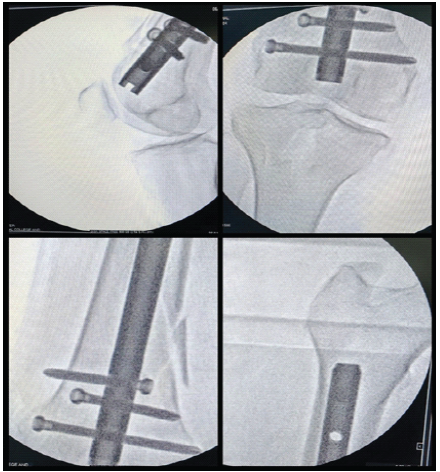
Figure 3: C-arm images showing retrograde nail in situ and proximal and distal locking.
A retrograde femoral nail appropriate for the canal size was then inserted. Distal locking was performed first to secure the short metaphyseal segment, followed by proximal locking. Final fluoroscopic images on both AP and lateral views showed acceptable overall alignment. No intraoperative adjuncts were required. The post-operative X-ray was radiologically acceptable and satisfactory.
The patient was mobilized with toe-touch weight bearing on the 1st post-operative day. At 4 weeks, radiographs showed maintained alignment (Fig. 4). By 2 months, callus was visible, and she progressed to full weight bearing (Fig. 5). Her functional recovery was in line with outcomes reported in the literature for retrograde nailing in osteoporotic distal femoral fractures [1,3,13,14].
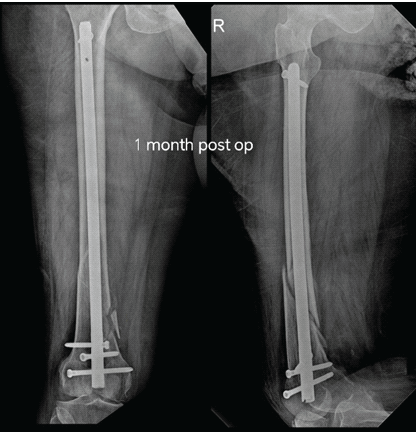
Figure 4: One month post-operative X-ray.
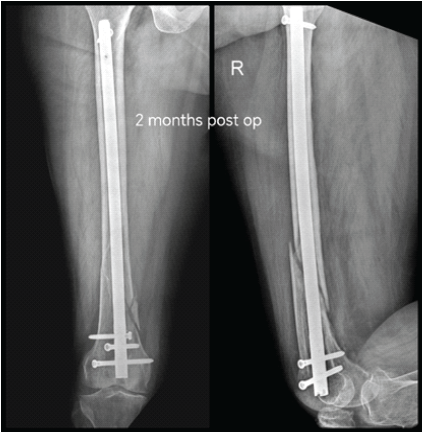
Figure 5: Two months post-operative X-ray.
Distal-third femoral shaft fractures in elderly osteoporotic patients are an awkward group to deal with. The bone is weak, the distal fragment is short, and the deforming forces are unforgiving. The canal flares proximally and tightens distally, and the distal segment has a tendency to fall into flexion and varus. Anyone who has dealt with these fractures knows that even a small loss of control early on can quickly turn into a major alignment problem. This is why, in most published series, surgeons do not hesitate to add toggler screws, cerclage wires, or temporary plates to hold the reduction, especially once reaming begins and the fragments start to drift [6,7]. Against that background, the present case is unusual because the reduction was achieved and maintained using indirect methods alone, without any mechanical assistance. Retrograde intramedullary nailing has been repeatedly shown to be a dependable option in elderly patients with osteoporotic distal femoral fractures, mainly because it shares load and preserves soft-tissue biology [1,2,3]. Kim et al. showed predictable union and acceptable function despite poor bone quality [1]. Canton et al. and Nam et al. also highlighted that in osteoporotic distal femur fractures, nails are often preferred over plates because they avoid periosteal stripping and reduce the risk of fixation failure in thin cortices [2,3]. These considerations were central to our decision-making. In an elderly patient with compromised bone stock, preserving biology and minimising additional trauma matters. What makes this case different is not the use of a retrograde nail. That is well established. It is the fracture pattern. Long-oblique distal-third fractures are inherently unstable, and the literature is clear about their tendency to lose reduction during guidewire passage or reaming [7,8,9,10]. Markmiller et al. described how fractures distal to an existing nail frequently displace during manipulation and often need additional stabilisation [8]. Ricci et al. pointed out that distal femur fractures, particularly in osteoporotic bone, behave unpredictably and are prone to failure if alignment is not secured early and reliably [7]. In many of these series, adjuncts were not an option. They were a necessity. In contrast, this case relied entirely on traction, rotational correction, soft-tissue tension, and continuous fluoroscopic monitoring. The fracture was not opened. No clamps, no collar screws, no cerclage, and no temporary plate. The reduction was allowed to occur through the limb’s own mechanics. This approach is very much in line with the principles described by Maniscalco and Regazzoni, who stressed the importance of respecting the soft-tissue envelope and using the limb’s natural elasticity to guide fragments into position rather than forcing alignment with hardware [15]. Their work may be older, but the principles remain relevant. Looking through available reports and small series on distal-third femur fractures treated with retrograde nails, two patterns stand out. First, most authors used some form of adjunct to hold the reduction, especially in metaphyseal or osteoporotic bone. Second, the fracture configurations were often transverse, short oblique, or comminuted rather than the long-oblique pattern seen here. Hartin et al., in their comparison of retrograde nails and fixed-angle plates for supracondylar fractures, still reported the need for intraoperative assistance to maintain alignment [6]. Müller et al. noted that long-oblique patterns behave differently and often push surgeons toward additional stabilisation to prevent drift [13]. Zlowodzki et al.’s meta-analysis echoed the same concern. Maintaining alignment during nailing is more difficult when the fracture line is long and sloping, with a tendency for rotational shear [12]. This is where the present case stands apart. The fracture was not only reduced indirectly, but the alignment was also maintained through the most vulnerable stage, which is reaming. That is where many reductions fail. Doing this without opening the fracture, without poller screws, without cerclage, and without temporary plating is not common, particularly in osteoporotic bone. The tendency of guidewire drift during reaming in osteoporotic metaphyseal bone and the need for sustained traction and continuous fluoroscopic reassessment are essential. In fact, the patient’s bone quality would usually push most surgeons in the opposite direction. Poor bone stock increases the risk of toggling and loss of control, which is why reduction aids are often added early [11]. Avoiding them here was not about proving a point. It was about respecting the limb’s natural alignment, allowing the soft tissues to relax, and not rushing into the canal before the fragments had truly settled. This case is a reminder of something that is slowly getting lost in modern trauma practice. Indirect reduction is a skill. It is not just a concept. When done patiently, with attention to detail and respect for the tissues, it can still work even in situations where many would default to mechanical assistance. The implant matters, but in difficult fracture patterns, the outcome often depends more on the technique and the discipline behind it than on the hardware itself. The authors acknowledge that the findings from this report cannot be generalised and should be interpreted within the limitations of a single-case experience. A biomechanical evaluation was beyond the scope of the present case report. Long-term assessment of alignment-related functional issues was not possible in this report. The described method may not be applicable to more complex fracture configurations requiring adjunctive stabilisation. Continuous fluoroscopic monitoring may not be equally practical in all surgical settings and may increase radiation exposure. The authors also accept that the technical demands of maintaining reduction during reaming and the importance of surgeon familiarity with indirect reduction principles have a long learning curve.
Pure indirect reduction, when performed patiently and with a clear understanding of the soft-tissue envelope, can still achieve stable alignment in an unstable distal-third femoral shaft fracture in osteoporotic bone. Retrograde intramedullary nailing remains a reliable option in this group, and this case shows that adjunctive reduction tools, while useful, are not mandatory in every scenario.
A stable axis in an unstable distal-third femoral shaft fracture can be achieved without poller screws or cerclage when meticulous indirect reduction principles are respected, and retrograde nailing is performed with control.
References
- 1. Kim J, Kang SB, Nam K, Rhee SH, Won JW, Han HS. Retrograde intramedullary nailing for distal femur fracture with osteoporosis. Clin Orthop Surg 2012;4:307-12. [Google Scholar] [PubMed]
- 2. Canton G, Giraldi G, Dussi M, Ratti C, Murena L. Osteoporotic distal femur fractures in the elderly: peculiarities and treatment strategies. Acta Biomed. 2019;90(1-S):25-32. [Google Scholar] [PubMed]
- 3. Nam DJ, Kim MS, Kim TH, Kim MW, Kweon SH. Fractures of the distal femur in elderly patients: Retrospective analysis of a case series treated with single or double plates. J Orthop Surg Res 2022;17:55. [Google Scholar] [PubMed]
- 4. Masih I, Mohsin S, Kumar KS, Sreeranga N. Retrospective study of clinical profile and outcome of patients with distal femoral fractures managed by retrograde nail in a tertiary-care hospital. Int J Orthop Sci 2020;6:983-6. [Google Scholar] [PubMed]
- 5. Paramesh NS, Munirathnaiah PK. A prospective study of retrograde nailing for distal third femoral shaft fractures. Int J Res Orthop 2021;7:1021-5. [Google Scholar] [PubMed]
- 6. Hartin NL, Harris I, Hazratwala K. Retrograde nailing versus fixed-angle blade plating for supracondylar femoral fractures: a randomised controlled trial. ANZ J Surg 2006;76:290-4. [Google Scholar] [PubMed]
- 7. Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk factors for failure of locked plate fixation of distal femur fractures: An analysis of 335 cases. J Orthop Trauma 2014;28:83-9. [Google Scholar] [PubMed]
- 8. Markmiller M, Konrad G, Südkamp N. Femoral shaft fracture distal to an antegrade nail: Treatment options and results. J Trauma 2000;49:722-8. [Google Scholar] [PubMed]
- 9. Kregor PJ, Stannard J, Zlowodzki M, Cole PA. Distal femoral fracture fixation utilising the less invasive stabilisation system (LISS). Oper Tech Orthop 2001;11:230-6. [Google Scholar] [PubMed]
- 10. Wiss DA, Watson JT, Johnson EE. Fractures of the distal femur: Operative treatment. Instr Course Lect 1994; 43:433-48. [Google Scholar] [PubMed]
- 11. McKoy BE, An YH. Implant fixation in osteoporotic bone: Scientific principles and clinical implications. J Orthop Surg (Hong Kong) 2000;8:66-77. [Google Scholar] [PubMed]
- 12. Zlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: Systematic review and meta-analysis. Arch Orthop Trauma Surg 2006;126:411-6. [Google Scholar] [PubMed]
- 13. Müller FJ, Nerlich M, Pfeifer KJ, Nerlich A. The role of intramedullary nailing in distal femur fractures. Eur J Trauma Emerg Surg 2015;41:401-6. [Google Scholar] [PubMed]
- 14. Ehlinger M, Ducrot G, Adam P, Bonnomet F. Distal femur fractures. Rev Prat 2012;62:831-7. [Google Scholar] [PubMed]
- 15. Maniscalco P, Rivera F, Bastiani L, Regazzoni P. Closed reduction of femoral shaft fractures: Role of the soft-tissue envelope and indirect reduction. Injury 2000;31 Suppl 3:C15-25. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery
July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density
June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density