
Meniscal ramp lesions are frequently associated with chronic ACL injuries and can contribute to persistent post-operative knee instability if left untreated. Routine arthroscopic evaluation of the posteromedial compartment during ACL reconstruction is essential for optimal surgical outcomes.
Dr. Suhail Ahmad Khanday, Department of Orthopaedics, Government Medical College, Anantnag, Jammu and Kashmir. E-mail: khandaysuhail88@gmail.com
Abstract
Introduction: Anterior cruciate ligament reconstruction (ACLR) is a common procedure done to regain knee stability, but even after the technical success of the operation, some patients still experience residual instability. Anterior cruciate ligament (ACL) injuries are regularly accompanied by meniscal ramp lesions, which concern the posteromedial meniscocapsular junction and can lead to a persistent anterior and rotational laxity in case of inadequate treatment. Whether ramp lesion repair could help in avoiding residual instability after ACLR is a controversial issue.
Materials and Methods: The proposed study is a prospective observational comparative study involving 50 participants who planned to undergo arthroscopic ACLR as a primary operation in a tertiary care unit. The findings during intraoperation were used to categorise the patients into two groups: Group A (ACLR and concomitant ramp lesion repair; n = 25) and Group B (isolated ACLR and no ramp lesion; n = 25). The Lachman test and pivot-shift test were used to measure post-operative knee stability, and the Lysholm Knee Scoring Scale and subjective International Knee Documentation Committee (IKDC) score at six months' follow-up were used to measure functional outcomes.
Results: Group A exhibited a high rate of post-operative knee stability, with 88% having a negative Lachman test in comparison to Group B (72%), with residual pivot-shift positivity being significantly low in Group A (16%) compared to Group B (40%) (P = 0.03). The ramp repair group also performed better in terms of functional outcomes, having a higher mean Lysholm score (93.6 ± 4.8 vs 88.9 ± 6.2) and a high percentage of normal IKDC scores (56 vs 32). The parameters of residual instability were much lower in patients who received ramp lesion repair.
Conclusion: Meniscal ramp lesion repair done together with ACLR enhanced substantially residual knee instability and short-term functional outcomes. This can be improved by systematic assessment and proper management of ramp lesions during ACLR to increase the stability of the knee post-surgery and maximise patient outcomes.
Keywords: Anterior cruciate ligament reconstruction, functional outcome, knee instability, meniscal ramp lesion, pivot-shift test.
One of the most common orthopaedic procedures is anterior cruciate ligament reconstruction (ACLR), aimed at restoring knee stability and functionality following the ligamentous trauma; however, a subgroup of patients continues to complain of certain rotational instability despite anatomically successful reconstruction, which is worrying [1] as it suggests that certain comorbid injuries are not detected and not managed. Among them, the meniscal ramp lesions, as longitudinal tears of the peripheral attachment of the anterior horn of the medial meniscus to the meniscocapsular or meniscotibial junction, have been of increasing importance as the causes of the postoperative instability and the high incidence of them in anterior cruciate ligament (ACL)-deficient knees [2]. The medial meniscus is the secondary knee stabiliser; it is extremely vital, particularly in the anterior tibial translation and rotational forces. The ACL is destroyed, and damage to its posterior horn has serious implications on the biomechanics of the knee [3]. The ramp lesions that are underdiagnosed and undertreated are the lesions that are not routinely observed during normal arthroscopic examination because they are in the rear position, and minimum lesions are observed using the regular anterior portals [4]. “Some biomechanical studies have demonstrated that ramp lesions, which have not been treated, result in more anterior laxity and internal tibial rotation despite ACLR and contribute to poor graft performance and contribute to chronic instability [5]. It has been reported that there is a high relationship between ramp lesions and chronic ACL injuries of a prevalence rate between 9% and 40%, which means ramp lesions are more likely to be experienced in case of delayed reconstruction due to repeated occurrences of instability [6]. Besides, the magnetic resonance imaging (MRI) is advantageous, although it is less sensitive to identify ram lesions, and this is where systematic arthroscopic examination of the posteromedial compartment is thought to be significant in ACLR [7]. Further discussion is in the treatment of ramp lesions, in which the stable lesions are spontaneously cured since the peripheral meniscus is vascular, unstable, or a complete tear has been found to be treated with successful surgery repair [8]. It has been reported that all-inside and inside-out arthroscopic repair techniques have shown good healing outcomes and biomechanical stability in the combination of these methods with ACLR [9]. The available clinical outcome research results indicate that patients undergoing combined ACLR and repair of ramp lesions experience higher post-operative knee stability, reduced grade of pivot shift, and improved functional scores compared to their counterparts receiving no ramp lesion repair [10]. Further, the lack of treatment of ramp lesions has also been cited as a potential risk factor that contributed to the failure of the graft, particularly in young and active individuals who require more functions of the reconstructed knee [11]. Although more and more evidence has been produced on the topic of repairing ramp lesions, there is still uncertainty in the practice of surgery, and there are no agreed-upon guidelines on indications, timing, and means of repair [12]. This is why it is necessary to carry out further research to offer some clarifications on the relevance of meniscal ramp lesion repair in the prevention of residual instability following ACLR. The importance of ramp lesions to the biomechanics and functional outcomes of the post-operative knee is an important aspect that should be taken into consideration in an attempt to streamline the surgical process to maximise patient satisfaction and reduce the chances of revisionary surgery. Despite increasing evidence regarding ramp lesion repair, uncertainty remains regarding its routine management during ACLR. Therefore, the present study was conducted to evaluate the role of meniscal ramp lesion repair in preventing residual instability and improving post-operative functional outcomes following ACLR [13].
Study design:
This multicentric prospective observational comparative study was conducted in the departments of orthopaedics of various tertiary care teaching hospitals equipped with advanced arthroscopic surgical facilities and postoperative rehabilitation services over a period of 18 months, including patient recruitment, surgical intervention, and follow-up evaluation. The study was designed to evaluate the role of meniscal ramp lesion repair in preventing residual instability after ACLR. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Participants:
Inclusion criteria:
- Patients with an age between 18 and 45 years
- Patients with a unilateral and confirmed ACL tear through clinical examination, accompanied by MRI
- Patients who underwent primary arthroscopic ACLR
- Patients who can give informed written consent and agree to follow-up protocol.
Exclusion criteria:
- Multiligamentous knee injuries
- Previous surgery on the affected knee
- Advanced osteoarthritis of the knee (Kellgren-Lawrence grade ≥2)
- Associated fractures around the knee joint
- Infectious or inflammatory knee pathology.
Study sampling:
Study participants were selected using a consecutive sampling method. The eligible patients who presented to the orthopedic outpatient department or emergency services during the study period and met the inclusion criteria were consecutively enrolled until a predefined sample size was achieved. This sampling strategy was selected to decrease selection bias and approximate the population under study to real-world clinical practice.
Study sample size:
The sample size of 50 patients was determined based on previous comparable studies, expected case availability, and study feasibility during the study period. The study was designed as an exploratory comparative observational study to evaluate post-operative stability and functional outcomes following ACLR with and without ramp lesion repair.
Study groups:
Participants were divided into two groups based on intraoperative arthroscopic findings. Group A included patients with ACL tears associated with meniscal ramp lesions who underwent simultaneous ramp lesion repair during ACLR. Group B included patients with isolated ACL tears without ramp lesions who underwent isolated ACLR. Group allocation was based on arthroscopic findings and was not randomised.
Study parameters:
The main outcome measures were a clinical test-based assessment of residual knee instability (Lachman test, anterior drawer test, and pivot-shift test). Secondary outcome measures were functional outcome measured by validated knee scoring systems (Lysholm Knee Scoring Scale and International Knee Documentation Committee [IKDC] subjective score). Other factors considered included patient demographics, mechanism of injury, interval to surgery, and intraoperative findings.
Study procedure:
Patients underwent arthroscopic ACLR and were placed under general or spinal anaesthesia following a standardised protocol for surgery. Initially, diagnostic arthroscopy was done to confirm an ACL tear as well as to determine any intra-articular pathology. The posteromedial compartment was systematically evaluated to identify ramp lesions. Patients with a ramp lesion also underwent arthroscopic repair of the lesions using an all-inside technique to repair the lesions with suture devices. The ACL was then reconstructed using hamstring tendon autograft with accurate tunnels and fixation. All patients underwent an early range of motion, progressive strengthening, and gradual return to activity according to a standardised rehabilitation protocol postoperatively.
Study data collection:
Data were collected using a structured pro forma designed specifically for the study. Pre-operative data comprised patient demographics, injury features, and baseline clinical findings. Details of intraoperative findings, including the presence/absence of ramp lesions and surgical procedures performed, were noted. Clinical evaluations and functional scores were recorded during routine post-operative follow-up. All clinical data were recorded by the treating orthopaedic team using a structured pro forma.
Data analysis:
The data collected were entered into Microsoft Excel and analysed using the Statistical Package for the Social Sciences software. We summarised demographic and clinical variables using measures of descriptive statistics, including mean, standard deviation, frequency, and percentage. Comparisons between the two groups were made using an independent t-test and Chi-square test as required. A P < 0.05 was considered statistically significant.
A total of 50 patients undergoing arthroscopic ACLR were included in the study and equally divided into Group A (ACLR with ramp lesion repair, n = 25) and Group B (isolated ACLR without ramp lesion, n = 25). The majority of patients were young adults aged 26–35 years, with a male predominance observed in both groups (Table 1).
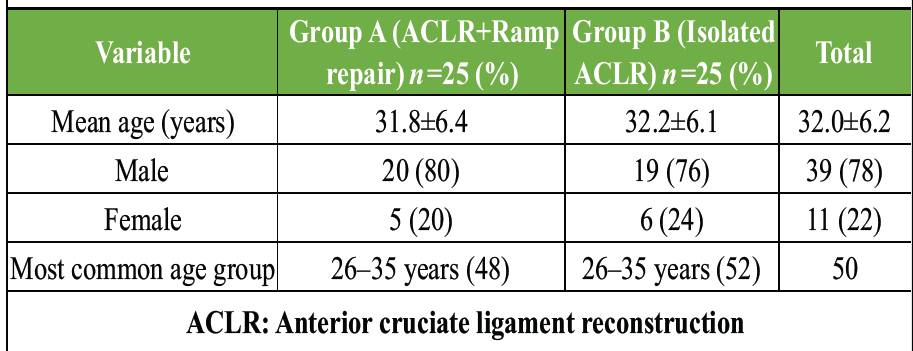
Table 1: Demographic characteristics of study participants
Sports-related injury was the most common mechanism of injury in both groups. Delayed surgery (>6 months from injury) was more frequently observed in patients with ramp lesions (64%) compared to isolated ACL injuries (40%) (Table 2 and Fig. 1).
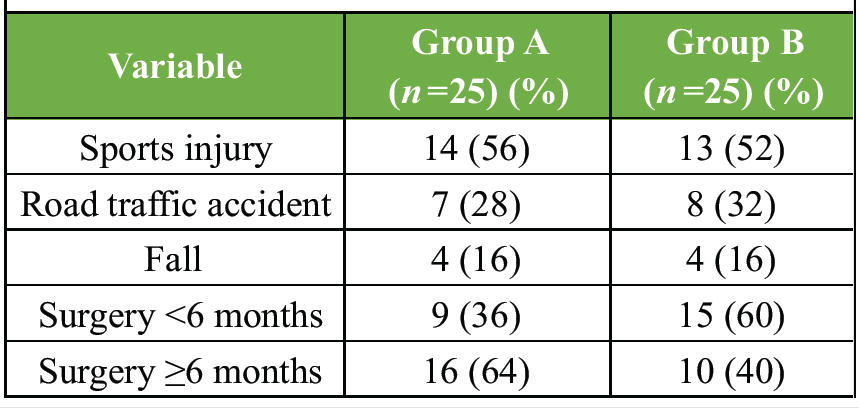
Table 2: Injury characteristics and time to surgery
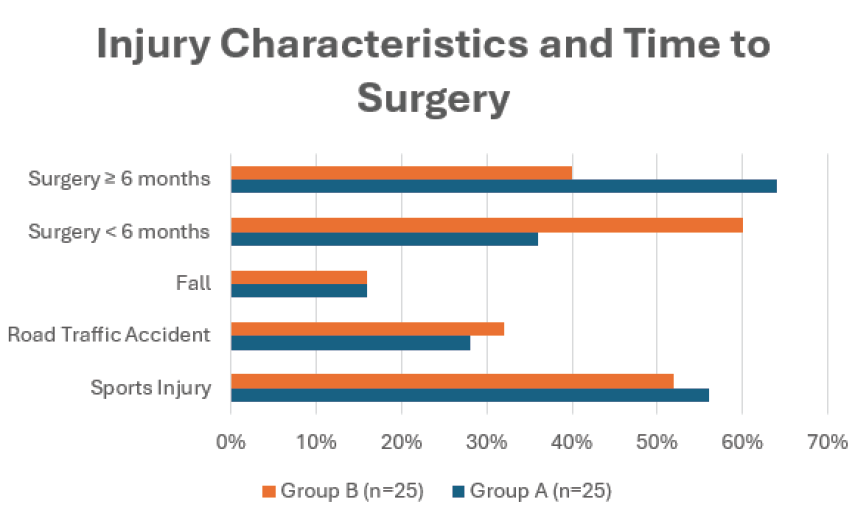
Figure 1: Injury characteristics and duration from injury to surgery among study groups.
Preoperatively, both groups demonstrated significant knee instability with positive Lachman and pivot-shift tests. At 6 months’ follow-up, Group A showed superior post-operative stability, with higher rates of negative Lachman test (88% vs. 72%) and negative pivot-shift test (84% vs. 60%) compared to Group B. Residual pivot-shift positivity was lower in Group A (16%) than Group B (40%) (P = 0.03) (Table 3 and Fig. 2).
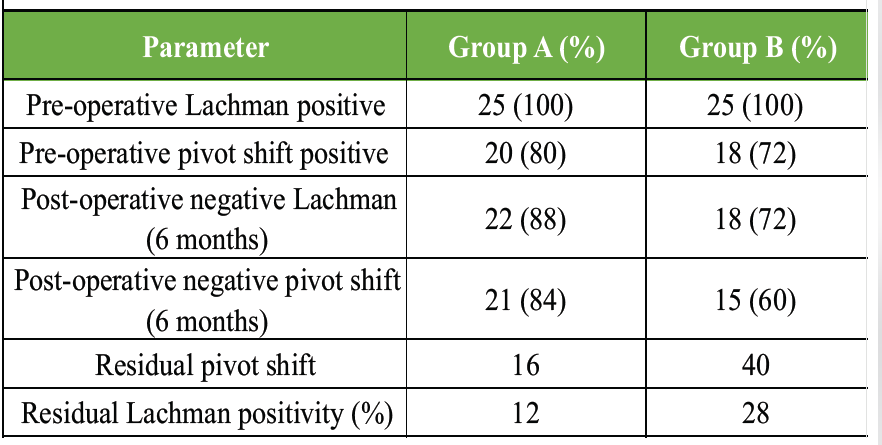
Table 3: Clinical instability tests (pre-operative and post-operative)
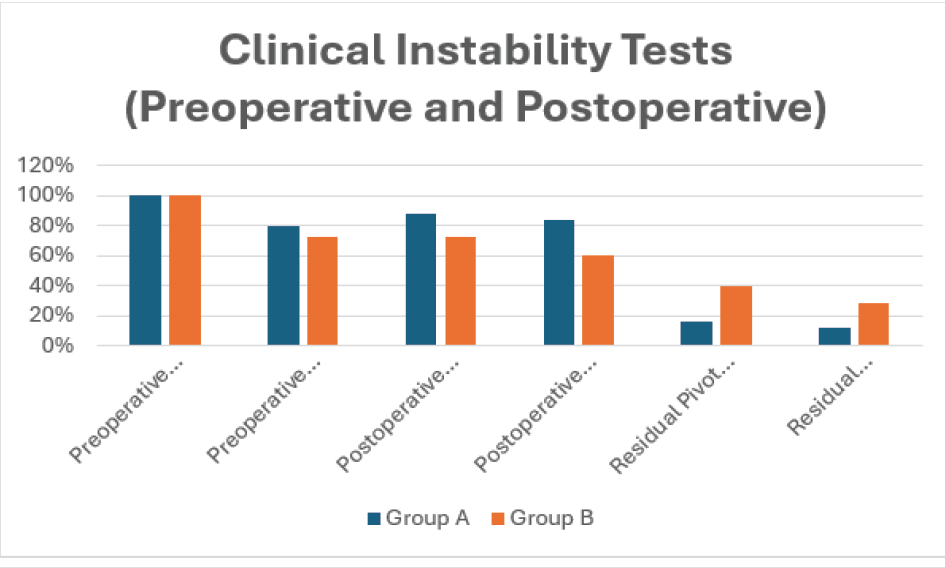
Figure 2: Comparison of pre-operative and post-operative instability tests between study groups.
Functional outcomes were better in patients undergoing ramp lesion repair. Group A demonstrated higher mean Lysholm scores compared to Group B (93.6 ± 4.8 vs. 88.9 ± 6.2). A greater proportion of patients in Group A achieved normal IKDC grades (56% vs. 32%), while abnormal IKDC grades were more common in Group B (24% vs. 8%) (Table 4).
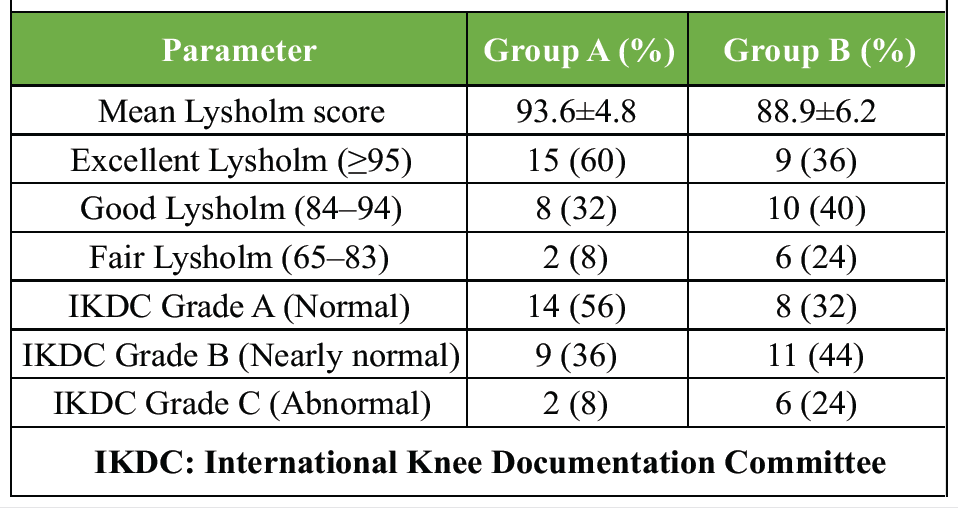
Table 4: Functional outcome scores at 6 months
The present study demonstrated that meniscal ramp lesion repair performed during ACLR improved post-operative knee stability and functional outcomes. Most patients were young male adults with sports-related injuries, reflecting the typical epidemiological pattern of ACL tears. Delayed surgery was more common in patients with ramp lesions, supporting the concept that chronic ACL deficiency predisposes to secondary meniscocapsular injury. Similar findings were reported by Hatayama et al. [14], who observed higher instability rates in patients with ramp lesions. Postoperatively, patients undergoing ramp lesion repair demonstrated better anterior and rotational stability, with lower residual Lachman and pivot-shift positivity compared to isolated ACLR. These findings support the biomechanical role of the posterior horn of the medial meniscus as a secondary stabiliser in ACL-deficient knees. Comparable biomechanical observations were reported by Li et al. [15], who demonstrated that ramp lesions increased anterior tibial translation and rotational instability, which improved following repair. Functional outcomes were also superior in the ramp repair group, with higher Lysholm scores and better IKDC grades compared to isolated ACLR. In contrast, Liu et al. [16] reported no significant difference between repaired and unrepaired stable ramp lesions. However, their study evaluated only stable lesions, whereas the present study compared repaired ramp lesions with knees without ramp pathology, which may explain the differing outcomes. The healing potential of ramp lesions has also been emphasised by DePhillipo et al. [17], who demonstrated superior healing rates in repaired lesions and improved post-operative stability in healed knees. Similarly, D’Ambrosi et al. [18] concluded that repair of unstable ramp lesions during ACLR improves knee function and stability. The findings of the present study further support the importance of systematic arthroscopic evaluation and appropriate management of ramp lesions during ACLR. The strengths of the present study include its prospective design, systematic arthroscopic assessment, and objective evaluation of post-operative instability and functional outcomes. However, limitations include the relatively small sample size, short follow-up duration, and lack of randomisation. Larger multicentric studies with longer follow-up are required to validate these findings.
Meniscal ramp lesion repair performed during ACLR improved post-operative knee stability and functional outcomes while reducing residual rotational laxity. Routine arthroscopic evaluation and appropriate management of ramp lesions during ACLR may improve post-operative knee stability and overall surgical outcomes.
Early identification and repair of meniscal ramp lesions during ACLR may improve post-operative rotational stability and functional recovery.
References
- 1. Bollen SR. Posteromedial meniscocapsular injury associated with rupture of the anterior cruciate ligament: A previously unrecognised association. J Bone Joint Surg Br 2010;92:222-3. [Google Scholar] [PubMed]
- 2. Chahla J, Moatshe G, Cinque ME, Godin J, Mannava S, LaPrade RF. Arthroscopic anatomic single-bundle anterior cruciate ligament reconstruction using bone-patellar tendon-bone autograft: Pearls for an accurate reconstruction. Arthrosc Tech. 2017;6:e1159-67. [Google Scholar] [PubMed]
- 3. Shoemaker SC, Markolf KL. The role of the meniscus in the anterior-posterior stability of the loaded anterior cruciate-deficient knee. Effects of partial versus total excision. J Bone Joint Surg Am 1986;68:71-9. [Google Scholar] [PubMed]
- 4. Stephen JM, Halewood C, Kittl C, Bollen SR, Williams A, Amis AA. Posteromedial meniscocapsular lesions increase tibiofemoral joint laxity with anterior cruciate ligament deficiency, and their repair reduces laxity. Am J Sports Med 2016;44:400-8. [Google Scholar] [PubMed]
- 5. Thaunat M, Fayard JM, Guimaraes TM, Jan N, Murphy CG, SonneryCottet B. Classification and surgical repair of ramp lesions of the medial meniscus. Arthrosc Tech 2016;5:e871-5. [Google Scholar] [PubMed]
- 6. Ziegler CG, Pietrini SD, Westerhaus BD, Anderson CJ, Wijdicks CA, Johansen S, et al. Arthroscopically pertinent landmarks for tunnel positioning in single-bundle and double-bundle anterior cruciate ligament reconstructions. Am J Sports Med 2011;39:743-52. [Google Scholar] [PubMed]
- 7. Parkinson B, Robb C, Thomas M, Thompson P, Spalding T. Factors that predict failure in anatomic single-bundle anterior cruciate ligament reconstruction. Am J Sports Med 2017;45:1529-36. [Google Scholar] [PubMed]
- 8. Di Vico G, Di Donato SL, Balato G, Correra G, D’Addona A, Maffulli N, et al. Correlation between time from injury to surgery and the prevalence of ramp and hidden lesions during anterior cruciate ligament reconstruction. A new diagnostic algorithm. Muscles Ligaments Tendons J 2017;7:491-7. [Google Scholar] [PubMed]
- 9. Edgar C, Kumar N, Ware JK, Ziegler C, Reed DN, DiVenere J, et al. Incidence of posteromedial meniscocapsular separation and the biomechanical implications on the anterior cruciate ligament. J Am Acad Orthop Surg 2019;27:e184-92. [Google Scholar] [PubMed]
- 10. Frank JM, Moatshe G, Brady AW, Dornan GJ, Coggins A, Muckenhirn KJ, et al. Lateral meniscus posterior root and meniscofemoral ligaments as stabilizing structures in the ACL-deficient knee: A biomechanical study. Orthop J Sports Med 2017;5:2325967117695756. [Google Scholar] [PubMed]
- 11. Geeslin AG, Civitarese D, Turnbull TL, Dornan GJ, Fuso FA, LaPrade RF. Influence of lateral meniscal posterior root avulsions and the meniscofemoral ligaments on tibiofemoral contact mechanics. Knee Surg Sports Traumatol Arthrosc. 2016;24:1469-77. [Google Scholar] [PubMed]
- 12. Goldsmith MT, Jansson KS, Smith SD, Engebretsen L, LaPrade RF, Wijdicks CA. Biomechanical comparison of anatomic single- and double-bundle anterior cruciate ligament reconstructions: An in vitro study. Am J Sports Med 2013;41:1595-604. [Google Scholar] [PubMed]
- 13. Papageorgiou CD, Gil JE, Kanamori A, Fenwick JA, Woo SL, Fu FH. The biomechanical interdependence between the anterior cruciate ligament replacement graft and the medial meniscus. Am J Sports Med 2001;29:226-31. [Google Scholar] [PubMed]
- 14. Hatayama K, Terauchi M, Saito K, Takase R, Higuchi H. Healing status of meniscal ramp lesion affects anterior knee stability after ACL reconstruction. Orthop J Sports Med 2020;8:2325967120917674. [Google Scholar] [PubMed]
- 15. Li S, Qin Y, Wang H, Qin Z, Jiang L, Zhu S, et al. Repair of ramp lesions of the medial meniscus with ACL reconstruction can better restore knee stability: A cadaveric study. Orthop J Sports Med 2023;11:23259671221140120. [Google Scholar] [PubMed]
- 16. Liu X, Zhang H, Feng H, Hong L, Wang XS, Song GY. Is it necessary to repair stable ramp lesions of the medial meniscus during anterior cruciate ligament reconstruction? A prospective randomized controlled trial. Am J Sports Med 2017;45:1004-11. [Google Scholar] [PubMed]
- 17. DePhillipo NN, Dornan GJ, Dekker TJ, Aman ZS, Engebretsen L, LaPrade RF. Clinical characteristics and outcomes after primary ACL reconstruction and meniscus ramp repair. Orthop J Sports Med 2020;8:2325967120912427. [Google Scholar] [PubMed]
- 18. D’Ambrosi R, Meena A, Raj A, Giorgino R, Ursino N, Mangiavini L, et al. Good results after treatment of RAMP lesions in association with ACL reconstruction: A systematic review. Knee Surg Sports Traumatol Arthrosc 2023;31:358-71.</p> [Google Scholar] [PubMed]
- 19. <p> [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes
May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes February 1, 2026 Arthroscopic Anterior Cruciate Ligament Reconstruction in a 17-Year-Old Female Athlete with Multiple Hereditary Exostoses Using a Peroneus Longus Autograft: A Rare Case Report
February 1, 2026 Arthroscopic Anterior Cruciate Ligament Reconstruction in a 17-Year-Old Female Athlete with Multiple Hereditary Exostoses Using a Peroneus Longus Autograft: A Rare Case Report February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes
February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study