
With this article, readers can understand the diagnosis and treatment of one possible complication of treating metacarpal fractures with percutaneous K-wires that, despite rare, can have a tremendous impact in outcomes.
Dr. Jorge Gomes Lopes, Department of Orthopaedics and Traumatology, Centro Hospitalar Universitário São João, Portugal. E-mail: j.andre.lp@gmail.com.
Abstract
Introduction: About 20% of all fractures in the human skeleton involves the hand, affecting primarily the young and active population. A Bennett’s fracture (BF) is a fracture of the base of the first metacarpal and surgical management is generally needed, with the K-wire fixation being the most preferred option. Among the most common complications with K-wires, we find infection and soft-tissues damages like tendon ruptures.
Case Report: Here, we report a case of iatrogenic rupture of the Little Finger’s Flexor Profundus Tendon after K-wire fixation of a BF that was diagnosed 4 weeks after the lesion. Different surgical strategies were proposed for managing chronic flexor tendon’s ruptures; however, no consensus exist around what option would be the best. Here, we describe a flexor transfer from the 5th to the 4th finger that resulted in a great improvement in patient’s DASH score and general quality of life.
Conclusion: It is important to remember that percutaneous fixations with K wires in the hand can have disastrous complications, patients should be evaluated for possible tendon ruptures after the surgery, no matter how impossible they may seem, as even unexpected complications can have easier solutions in the acute setting.
Keywords: Bennett’s Fracture, Complications, Tendon rupture, Tendon Repair, Tendon Transfer.
About 20% of all fractures in the human skeleton involve the hand, affecting primarily the young and active population [1]. The Bennett’s Fracture (BF) is an intra-articular injury that occurs at the proximal aspect of the thumb metacarpal and is the most common fracture involving the carpometacarpal joint [2]. There is still controversy around the best treatment option. No consensus has been reached regarding the long-term clinical benefits of an anatomic reduction, although it seems that articular step-offs exceeding 2 mm can lead to malunion and consequently joint subluxation and arthritis [1,3]. Surgical management is generally advocated and popular surgical techniques include close reduction and fixation with Kirschner wires (K-wire) or open reduction and internal fixation, with screws and/or plates, often followed by cast immobilization [2,3]. Although it is a popularized technique, K-wire complications are not uncommon. Pin tract infection and K-Wire migration are the most frequently reported. Although the majority is easily treated, some can lead to catastrophic results [4]. Tendon rupture as a consequence of K-wire placement for BF’s fixation is rare and few have been described in the literature [5]. Direct tendon piercing and rupture or abrasion are among the possible causes [6]. Most patients with injured flexor tendons do well after primary repair but some present for treatment so late that primary repair is not possible anymore. Despite some controversies, surgical treatment is the most acceptable option to restore function, but we still do not have a consensus about the preferred technique [6,7]. When it comes to the little finger, bridge tendon graft, end-to-side tendon transfer using the flexor digitorum profundus (FDP) of another finger, or even inter-phalangeal arthrodesis are all options to consider [6]. Here, we describe an iatrogenic rupture of the FDP of the fifth finger after percutaneous fixation of a BF, treated with an end-to-side tendon transfer, using the FDP of the ring finger, archiving good range of motion and restoring function completely.
We report a case of a 44-year-old physical education teacher that was involved in a car accident in June of 2021. He was admitted in the emergency department right after the accident and a fracture of the base of the first metacarpal with partial articular involvement (Bennett fracture) was diagnosed Fig. 1.Patient’s hand and wrist were immobilized in a cast for pain management and surgery was scheduled for the day after. Closed reduction and internal fixation with two 1.5 mm K-wires were the strategy chosen and the patient was maintained in a cast for 4 weeks with X-ray monitoring at 1st-and 3rd-week post-operative. There is no reports of intra or post-operative neurovascular complications and serial X-rays revealed no loss of reduction. At the 4th week, because of insurances motifs, the patient changed medical institutions. By that time, there was signs of consolidation on X-ray and K-wires were removed.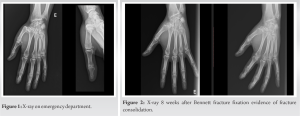 The physical evaluation on removal of the K-wires denoted a deficit of fifth5th finger distal interphalangeal (IP) active flexion, no sensitive deficits and no complaints on passive flexion. Patient clearly stated that he had no flexion limitation after the trauma and before the surgery but he did not notice any alteration while immobilized in a cast. There was no fracture on the X-ray besides the Bennett fracture and ultrasound evaluation described a rupture of the FDP of the fifth finger on flexor’s zone IV with no visible proximal stump. The superficial flexor was apparently intact, as well as the tendons of the other four fingers. Therapeutic options were discussed with the patient and he emphasized the importance of distal IP flexion in is job. Eight weeks after fracture fixation, consolidation could be documented on X-ray (Fig. 2) and a surgical strategy addressing tendon rupture was proposed. Patient was unreceptive to tendon allograft or autograft options but it was explained that palmaris longus tendon might be needed for the repair. By this time, there was no flexion of the distal IP joint of the little finger Fig. 3a and b, wrist flexion and extension was approximately 60° each, radial deviation was around 15°. Opposition Kapandji grade was 5 and DASH score was 48.3. A Bruner’s incision on Zone III and IV was performed and the distal stump was individualized but there was no sign of the proximal one in all zone IV. The tendon was too retracted for an adequate direct repair.
The physical evaluation on removal of the K-wires denoted a deficit of fifth5th finger distal interphalangeal (IP) active flexion, no sensitive deficits and no complaints on passive flexion. Patient clearly stated that he had no flexion limitation after the trauma and before the surgery but he did not notice any alteration while immobilized in a cast. There was no fracture on the X-ray besides the Bennett fracture and ultrasound evaluation described a rupture of the FDP of the fifth finger on flexor’s zone IV with no visible proximal stump. The superficial flexor was apparently intact, as well as the tendons of the other four fingers. Therapeutic options were discussed with the patient and he emphasized the importance of distal IP flexion in is job. Eight weeks after fracture fixation, consolidation could be documented on X-ray (Fig. 2) and a surgical strategy addressing tendon rupture was proposed. Patient was unreceptive to tendon allograft or autograft options but it was explained that palmaris longus tendon might be needed for the repair. By this time, there was no flexion of the distal IP joint of the little finger Fig. 3a and b, wrist flexion and extension was approximately 60° each, radial deviation was around 15°. Opposition Kapandji grade was 5 and DASH score was 48.3. A Bruner’s incision on Zone III and IV was performed and the distal stump was individualized but there was no sign of the proximal one in all zone IV. The tendon was too retracted for an adequate direct repair. 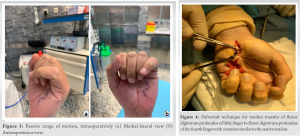 The distal stump of the FDP tendon of the little finger was woven through the FDP tendon of the ring finger (pulvertaft suture with 3 loops) and sutured with non-absorbable monofilament, in the same tension as that of the resting position of the unaffected little finger Fig. 4. As the rupture was in zone IV, we had a proximal stump of a considerable length so that it could be sutured as proximal as possible to approximate the gliding direction of the original FDP tendon of the little finger. A dorsal plaster splint was used to immobilize the hand and wrist in the neutral position, keeping the metacarpophalangeal (MP) joints at around 50° of flexion and the IP joints at 0° of flexion. Passive and active gentle flexion was encouraged, several times a day, from the 1st-day post-operative and extension was allowed in the limits of the splint. The dorsal splint was discontinued during the day after 6 weeks and completely removed by the 8th week. Rehabilitation, 4 days a week, was maintained for another 4 weeks. At the 12th-week post-operative, the range of motion of both little and ring fingers were complete (full extension and full flexion of MP and Ips joints) (Fig. 5a and b); DASH score was 23.2 points.
The distal stump of the FDP tendon of the little finger was woven through the FDP tendon of the ring finger (pulvertaft suture with 3 loops) and sutured with non-absorbable monofilament, in the same tension as that of the resting position of the unaffected little finger Fig. 4. As the rupture was in zone IV, we had a proximal stump of a considerable length so that it could be sutured as proximal as possible to approximate the gliding direction of the original FDP tendon of the little finger. A dorsal plaster splint was used to immobilize the hand and wrist in the neutral position, keeping the metacarpophalangeal (MP) joints at around 50° of flexion and the IP joints at 0° of flexion. Passive and active gentle flexion was encouraged, several times a day, from the 1st-day post-operative and extension was allowed in the limits of the splint. The dorsal splint was discontinued during the day after 6 weeks and completely removed by the 8th week. Rehabilitation, 4 days a week, was maintained for another 4 weeks. At the 12th-week post-operative, the range of motion of both little and ring fingers were complete (full extension and full flexion of MP and Ips joints) (Fig. 5a and b); DASH score was 23.2 points. 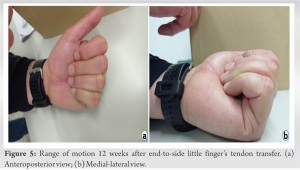 We felt that most of patient’s limitations at that moment came from the residual pain at the first metacarpal base and were in agreement with what was expected from the natural course of the fracture. By this time, the patient was allowed to return to work with light duty restrictions and 4 weeks later, he was able to work with no limitations.
We felt that most of patient’s limitations at that moment came from the residual pain at the first metacarpal base and were in agreement with what was expected from the natural course of the fracture. By this time, the patient was allowed to return to work with light duty restrictions and 4 weeks later, he was able to work with no limitations.
K-wires have been widely used for fixation of radius and hand fractures after close reduction [4]. Complications are usually related to soft-tissue injury, as wires can damage tendons or neurovascular structures, or infections around the wire [5]. Iatrogenic injuries after distal radius fixation are extensively described in the literature and every orthopedic surgeon is promptly aware of it. On the other hand, reports on soft-tissues complications after fixation of carpal or metacarpal bones fractures is harder to find. Percutaneous stabilization of an intra-articular fracture of the base of the first metacarpal consists in joining the first metacarpal and its fragments to the trapezium bone and/ or adjacent metacarpals [3]. Conventionally, wires are placed through certain “safe zones” where direct risk of soft-tissue injury can be kept to a minimum. However, they may also cause damage by abutting structures which, in turn, leads to attritional extensor tendon ruptures or disabling neuritis [5]. Milliez et al. suggested that early mobilization of the wrist with pins in place increased the likelihood of tendon rupture as they found increased wire migration and tendon rupture in a group of patients that were mobilized soon after pinning [8]. In the described case, the patient denied any limitations previous to surgery and the rupture was already present when the cast was removed which may indicate that it was caused by direct piercing of the tendon. Flexor tendon ruptures, especially when both superficial and profundus tendons are cut, are disabling hand lesions that have a tremendous impact on a patient’s quality of life, limiting even simple daily life activities. Treating chronic ruptures is always a challenge to the hand surgeon. It not only relies on the type of lesion or the elapsed time, but also on patient’s age, motivation, rehabilitation compliance, and comorbidities, which play an important role in the potential for biological repair [7]. After 3 weeks from the lesion, primary tendon repair may not be feasible [9]. Free gliding of the tendons within the digital canal is fundamental and adhesions or dense scar tissue frequently limit the success of this strategy [7]. Proximal end retraction often leads to excessive tension on the repaired tendon which makes it prone to failure [10]. However, this decision is only possible during surgery and both surgeon and patient should always be prepared for alternatives. Grafting of flexor tendons has also become a popular treatment when the integrity of the tendon is compromised though it is demanding, often requiring multiple stage surgeries, the rates of complications and failures are high and add donor site morbidity [11]. Active tendon implants are an alternative in reconstructive flexor tendon surgery and are indicated for patients with a poor prognosis or in whom the classical techniques failed [7]. When a redundant tendon with low donor site morbidity is available for transfer, tendon transfer may be a better option compared to tendon grafting as it avoids a potentially incompetent proximal muscular unit and, in the end, there is only one site of repair to heal [12]. Conservative measures in cases of isolated little finger FDP rupture can lead to acceptable function and minimal disability and it is often argued that tendon reconstruction should be reserved for individuals with occupations requiring active distal IP flexion [13]. It was both ours and patient’s understanding that a physical education professor demanded distal IP flexion for innumerous activities making him a candidate for surgical treatment. In FDP tendon reconstruction, the tendon graft is often secured to the adjacent, intact FDP tendon, and not to the proximal FDP stump, creating a coupled digital motion and eliminating any functional independence between the adjacent fingers [14]. Tendon transfer with side-to-side, end-to-side, or pulvertaft suture is a common procedure with good results in FDP ruptures in rheumatoid hands [12,15]. Our patient’s FDP tendon of the small finger was deemed unfit for direct repair. The proximal stump was too retracted, could not be found close to the distal one, and exploration would demand an unacceptable long surgical incision. We were also not willing to cause donor site morbidity and therefore decided to go with a tendon transfer with side-to-side suture of the distal stump of FDP of the fifth finger to the FDP of the fourth finger. This strategy was already found to produce similar outcomes to bridge tendon grafts in terms of total active motion and grip strength without major complications [6]. After 4 months of rehabilitation, range of motion was complete and the patient was satisfied with the result.
This is a representative case of a known complication with a rare anatomic location. Iatrogenic tendon ruptures after K-wire fixation can easily become chronic as patients may stay for a while in a cast. If the ruptured tendon is the least expected, the probability of detecting it without a thorough inspection is even lower. When it comes to isolated FDP rupture, the literature is limited to a few case series and expert opinions with no comparisons of the surgical and nonsurgical treatment or the various surgical techniques. The surgeon must be familiar with different treatment options and discuss with the patient his expectations and accomplishable results. The chosen treatment is an option to achieve patient’s satisfaction without causing additional morbidity and we should have this strategy in mind.
Despite, iatrogenic ruptures of hand tendons, having already been extensively described, the literature focuses, almost exclusively, on distal radius fractures. We, as surgeons, should be equally aware of this complication while fixing hand fractures and any suspicion of limited finger function, independently of the anatomic improbability, should prompt a careful inspection. Moreover, we should train ourselves for a close follow-up of all tendons function during the initial post-operative period, especially, the first few days.
References
- 1.Varitimidis S, Dailiana Z, Agorastakis D, Fyllos A, Zibis A, Hantes M, et al. Long-term functional results of intra-and extra-articular hand fractures treatment with titanium miniature plates and screws with minimum follow-up of 24 months. Cureus 2021;13:e15438. [Google Scholar | PubMed]
- 2.Yin Y, Wang Y, Wang Z, Qu W, Tian W, Chen S. Accuracy of fluoroscopic examination in the treatment of Bennett’s fracture. BMC Musculoskelet Disord 2021;22:3. [Google Scholar | PubMed]
- 3.Levy V, Mazzola M, Gonzalez M. Intra-articular fracture of the base of the first metacarpal bone: Treatment through a volar approach. Hand (N Y) 2018;13:90-4. [Google Scholar | PubMed]
- 4.Subramanian P, Kantharuban S, Shilston S, Pearce OJ. Complications of Kirschner-wire fixation in distal radius fractures. Tech Hand Up Extrem Surg 2012;16:120-3. [Google Scholar | PubMed]
- 5.Kirmani SJ, Bhuva S, Lo W, Kumar A. Extensor tendon injury to the index and middle finger secondary to Kirschner wire insertion for a distal radial fracture. Ann R Coll Surg Engl 2008;90:W14-6. [Google Scholar | PubMed]
- 6.Kuroda T, Moriya K, Tsubokawa N, Maki Y, Inagaki K, Yoshizu T. Comparison of bridge graft and end-to-side transfer for treatment of closed rupture of the flexor tendons in the little finger. J Hand Surg Eur Vol 2022;47:520-6. [Google Scholar | PubMed]
- 7.Battiston B, Triolo PF, Bernardi A, Artiaco S, Tos P. Secondary repair of flexor tendon injuries. Injury 2013;44:340-5. [Google Scholar | PubMed]
- 8.Milliez PY, Dallaserra M, Defives T, El Ayoubi L, Thomine JM. Effect of early mobilization following Kapandji’s method of intrafocal wiring in fractures of the distal end of the radius. Results of a prospective study of 60 cases. Int Orthop 1992;16:39-43. [Google Scholar | PubMed]
- 9.Griffin M, Hindocha S, Jordan D, Saleh M, Khan W. An overview of the management of flexor tendon injuries. Open Orthop J 2012;6:28-35. [Google Scholar | PubMed]
- 10.Tang JB. Uncommon methods of flexor tendon and tendon-bone repairs and grafting. Hand Clin 2013;29:215-21. [Google Scholar | PubMed]
- 11.Finsen V. Two-stage grafting of digital flexor tendons: A review of 43 patients after 3 to 15 years. Scand J Plast Reconstr Surg Hand Surg 2003;37:159-62. [Google Scholar | PubMed]
- 12.O’Sullivan MB, Singh H, Wolf JM. Tendon transfers in the rheumatoid hand for reconstruction. Hand Clin 2016;32:407-16. [Google Scholar | PubMed]
- 13.Birman MV, Strauch RJ. Management of late-presenting isolated flexor digitorum profundus injuries. J Hand Surg Am 2012;37:1065-7. [Google Scholar | PubMed]
- 14.Morrell NT. The FDP-FDS-FDP dual tendon transfer: A simple, single-stage reconstruction technique for chronic, isolated flexor digitorum profundus tendon injuries. Tech Hand Up Extrem Surg 2019;23:62-4. [Google Scholar | PubMed]
- 15.Schindele SF, Herren DB, Simmen BR. Tendon reconstruction for the rheumatoid hand. Hand Clin 2011;27:105-13. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Vascularized First Dorsal Metacarpal Artery-Based Adipofascial Flap to Augment Multiple Zone VII Extensor Tendon Repairs after Glass Laceration: A Case Report
July 1, 2026 Vascularized First Dorsal Metacarpal Artery-Based Adipofascial Flap to Augment Multiple Zone VII Extensor Tendon Repairs after Glass Laceration: A Case Report June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study
June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study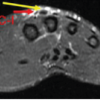 June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report May 1, 2026 Segmental Achilles Tendon Loss With Skin Defect in an Open Calcaneal Fracture Managed Without Tendon Reconstruction: A Case Report
May 1, 2026 Segmental Achilles Tendon Loss With Skin Defect in an Open Calcaneal Fracture Managed Without Tendon Reconstruction: A Case Report