
In cases of intertrochanteric fractures, clinicians should consider potential vascular damage if a patient exhibits ongoing thigh edema and unresolved post-operative anemia.
Dr. Anant Kumar Singh, Department of Orthopaedic Surgery, Dr. R. L. Hospital, Raigarh Chhattisgarh, India. E-mail: anantsingh37@gmail.com
Abstract
Introduction: Pseudoaneurysm of the medial femoral circumflex artery is a rare but potentially serious vascular complication following surgical fixation of trochanteric femur fractures. It may present with thigh swelling, anaemia, or persistent pain and can be easily overlooked in the postoperative period.
Case Report: We report a case of medial femoral circumflex pseudoaneurysm developing after internal fixation of an intertrochanteric femur fracture. The diagnosis was confirmed using colour Doppler and successfully treated with exploration and ligation.
Conclusion: Early recognition and prompt management are essential to avoid life-threatening complications.
Keywords: Pseudoaneurysm, intertrochanteric fracture, proximal femoral nail.
Trochanteric fractures of the femur are common injuries, especially in elderly patients, and are typically treated with internal fixation using devices such as dynamic hip screws or proximal femoral nails [1]. Although these procedures are generally safe, vascular complications may occasionally occur [2,3]. Pseudoaneurysm of the profunda femoris artery and its branches is an uncommon but important complication, having a reported incidence of 0.2–0.49% [4]. Several factors may be contributing to its occurrence, including sharp displaced bone fragments, misdirected screws, over-penetration during drilling, or improper placement of retractors and bone levers. In addition to these, limb positioning during surgery, excessive adduction, internal rotation, or traction, or a large perineal post may contribute to increasing the risk of vascular compromise, particularly to the profunda femoris artery and its branches [4]. Because symptoms may be delayed and non-specific, diagnosis can be challenging, and delayed recognition may lead to significant morbidity. The most common presenting symptoms could be pain and swelling over the proximal thigh with associated lower limb edema. Given the diagnostic challenge and life-threatening consequence, the treating surgeon should maintain a high index of suspicion while treating a peritrochanteric fracture in the postoperative period [5]. We report a case of medial circumflex artery pseudoaneurysm following surgical fixation of a trochanteric fracture with proximal femoral nail Antirotation II.
A 65-year-old male presented to the emergency department following a fall from standing height, complaining of pain and inability to bear weight on his right lower limb. On examination, there was shortening of the limb and external rotation along with tenderness and fullness over the groin and a restricted range of movement of the hip. Radiographs revealed an intertrochanteric fracture of the right femur, Boyd and Griffin Type II (Fig. 1a). The patient underwent surgical fixation using a proximal femoral nail under spinal anaesthesia. The procedure was uneventful, and post-operative radiographs confirmed satisfactory fracture reduction and implant placement (Fig. 1b).
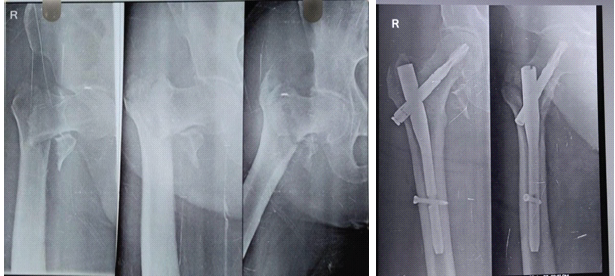
Figure 1: preop x ray and immediate post op
The post-operative period was uneventful, and he was discharged on the 5th post-operative day. The patient was mobilised on a walker with partial weight bearing, and sutures were removed on the 14th postoperative day with the surgical scar dry and healthy. In the 4 postoperative weeks, the patient developed progressive swelling of the proximal thigh associated with persistent pain. Clinical examination revealed tense swelling over the lateral thigh without signs of wound infection. Pitting oedema was present. Distal pulses were palpable. However, the patient showed a progressive drop in haemoglobin levels despite no obvious external bleeding. Ultrasonography with Doppler revealed a vascular lesion suggestive of a pseudoaneurysm measuring approximately 2.5 cm originating from a branch of the profunda femoris artery. Preoperative computed tomography (CT) angiography was not performed as the patient deteriorated haemodynamically. The patient was referred to the cardiothoracic and vascular surgery team, and immediate exploration of the femoral artery along with its branches was done, which revealed a loose bony fragment causing a pseudoaneurysm (size 4 × 5 cm) of the medial circumflex artery branch of the profunda femoris artery, which was explored, debrided, and ligated with the removal of the bony fragment. Following the procedure, the patient showed rapid clinical improvement, showing a reduction in thigh swelling and stabilisation of haemoglobin levels. The post-operative recovery was uneventful, and the patient was discharged with instructions for follow-up. At the 3-month follow-up visit, the fracture was progressing toward union, and the patient had no vascular symptoms.
A pseudoaneurysm develops when arterial integrity is compromised, causing blood to escape and form a fibrous capsule containing a haematoma that remains in communication with the main artery. Unlike a true aneurysm, a pseudoaneurysm lacks all arterial walls, making it prone to expansion, rupture, and secondary complications such as infection, neurovascular compression, ischaemia, and pain [3,5,6]. The profunda femoris artery originates from the posterolateral aspect of the femoral artery approximately 3 cm below the inguinal ligament. It travels medially and posteriorly along the thigh, giving rise to the medial and lateral circumflex femoral artery, and continues through the adductor muscles to supply the posterior compartment of the thigh through its perforating branches [7]. Pseudoaneurysm of the medial femoral circumflex artery is a rare complication following hip fracture surgery. The medial femoral circumflex artery lies near the femur, making it vulnerable to injury during fracture or surgical intervention. Several mechanisms have been proposed for vascular injury, including penetration by drill bits or screws, over-penetration of cortical drilling, injury from displaced fracture fragments, and retraction or manipulation during surgery [8]. Clinical presentation can vary. Patients may present with thigh swelling, persistent pain, pulsatile mass, unexplained anaemia, or delayed wound bleeding. Because symptoms are often non-specific, a high index of suspicion is necessary. In our case, the likely cause of pseudoaneurysm was the displaced lesser trochanter fragment as identified during the exploration and suggested by the anatomical correlation. (Fig. 2 with clinical picture)
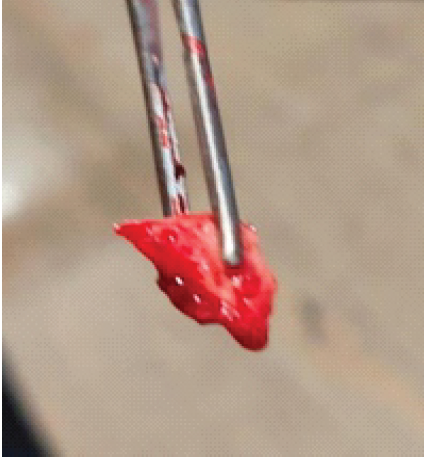
Figure 2:Removed bony fragment causing pseudoaneurysm
Persistence of progressive pulsatile swelling and unexplained anaemia should have prompt early vascular evaluation. Early Doppler (Fig. 3) identified the collection; however, sudden clinical and haemodynamic deterioration didn’t allow further evaluation by CT angiography, and clinical exploration was performed, thereby identifying and treating the pseudoaneurysm and avoiding the catastrophic complications, including rupture and haemorrhagic shock.
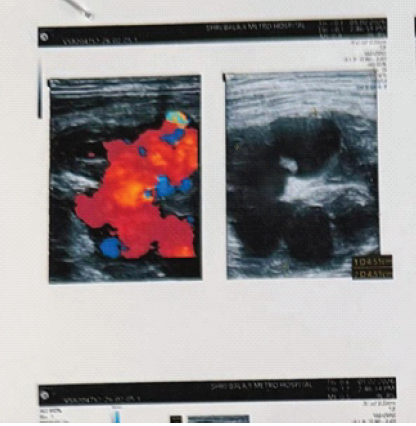
Figure 3: Pre op colour doppler
Contrast-enhanced CT scanning and angiography are considered the gold standard for diagnosis; however, duplex and color Doppler ultrasounds are excellent for confirming the diagnosis with a sensitivity and specificity of 97% and 93%, respectively [9]. Transcatheter arterial embolisation is a less invasive treatment than surgery, but surgical exploration, resection, and ligation may be necessary in cases in unstable general conditions or urgent thigh decompression [10]. As in our case, the surgeon opted for immediate exploration and decompression, as the general condition was unstable. Occurrence of scalloping on the medical femoral cortex on X-ray can be an important finding to suspect PA, in addition to a pulsatile mass on the medial side of the thigh [11]. However, we observed a lytic lesion over the greater trochanter (Fig. 4), which was not evident in the immediate postoperative period.

Figure 4:post op xray after 1 month with GT lysis
The collection and pressure effect of the pseudoaneurysm were more over the greater trochanter, we assume, which resulted in the bony erosion of the greater trochanter. Similar radiographic findings in the form of scalloping in the medial femoral cortex have been reported by Vande Voorde et al. [12]. A high degree of suspicion, timely recognition, and proper investigation could prevent catastrophic complications in cases of post-operative PA cases.
Pseudoaneurysm of the medial femoral circumflex artery is a rare but important vascular complication following surgical fixation of trochanteric femur fractures.
Persistent thigh swelling and unexplained post-operative anemia should raise suspicion of vascular injury in intertrochanteric fracture. Early imaging and endovascular management can lead to excellent outcomes.
References
- 1. Peeters CM, Visser E, Van De Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after hip fracture in the elderly: A systematic literature review. Injury 2016;47:1369-82. [Google Scholar] [PubMed]
- 2. De Raaff CA, Van Nieuwenhuizen RC, Van Dorp TA. Pseudoaneurysm after pertrochanteric femur fracture: A case report. Skeletal Radiol 2016;45:575-8. [Google Scholar] [PubMed]
- 3. Yoon HK, Oh HC, Park J, Oyunbat C, Kim T. Rupture of the deep femoral artery during proximal femoral nailing following an intertrochanteric fracture: A case report. Hip Pelvis 2016;28:54-9. [Google Scholar] [PubMed]
- 4. Samaan M, Idres FA, Hawa Y, Madania M. Late deep femoral artery injury after intertrochanteric hip fracture treatment: A case report. Int J Surg Case Rep 2023;105:107983. [Google Scholar] [PubMed]
- 5. Kulkarni SL, Daragad M, Ravikiran R, Manoj N. A rare case of pseudoaneurysm of profunda femoris artery following surgical fixation of an intertrochanteric fracture. J Orthop Case Rep 2025;15:174-8. [Google Scholar] [PubMed]
- 6. Murata K, Nagira K, Ishida K, Hayashi I, Okuno M, Nagashima H. Pseudoaneurysms after osteosynthesis of hip fracture: A report of two cases and a review of the literature. JOS Case Rep 2023;2:113-7. [Google Scholar] [PubMed]
- 7. Ginzburg E, Chong CK, Rich NM. Vascular anatomy of the extremities. In: Asensio JA, Trunkey DD, editors. Current Therapy of Trauma and Surgical Critical Care. St. Louis: Mosby; 2008. p. 467-72. [Google Scholar] [PubMed]
- 8. Barquet A, Gelink A, Giannoudis PV. Proximal femoral fractures and vascular injuries in adults: Incidence, aetiology and outcomes. Injury 2015;46:2297-313. [Google Scholar] [PubMed]
- 9. Fernandez Gonzalez J, Terriza M, Cabada T, Garcia-Araujo C. False aneurysm of the femoral artery as a late complication of an intertrochanteric fracture. A case report. Int Orthop 1995;19:187-9. [Google Scholar] [PubMed]
- 10. Chan WS, Kong SW, Sun KW, Tsang PK, Chow HL. Pseudoaneurysm and intramuscular haematoma after dynamic hip screw fixation for intertrochanteric femoral fracture: A case report. J Orthop Surg (Hong Kong) 2010;18:244-7. [Google Scholar] [PubMed]
- 11. Arbeloa-Gutierrez L, Arenas-Miquelez A, Munoa L, Gordillo A, Eslava E, Insausti I, et al. Lateral circumflex femoral artery false aneurysm as a complication of intertrochanteric hip fracture with displaced lesser trochanter. J Surg Case Rep 2019;2019:rjz184. [Google Scholar] [PubMed]
- 12. Vande Voorde K, Dauwe J, Van Oost J. Late presentation of an iatrogenic pseudoaneurysm of the profunda femoris artery following intramedullary nailing. Case Rep Orthop 2018;2018:8270256. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study
August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report
June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report November 1, 2025 Impact of Tip Apex Distance, Cortical Reduction, and Lateral Wall Integrity on Radiological Union of Unstable Trochanter Fracture Treated with Proximal Femoral Nail: A Retrospective Observational Study
November 1, 2025 Impact of Tip Apex Distance, Cortical Reduction, and Lateral Wall Integrity on Radiological Union of Unstable Trochanter Fracture Treated with Proximal Femoral Nail: A Retrospective Observational Study