
In isolated medial compartment osteoarthritis, both high tibial osteotomy (HTO) and unicompartmental knee arthroplasty (UKA) effectively reduce pain and improve function. However, UKA demonstrates superior functional outcomes and range of motion (ROM), making it a preferred option in appropriately selected patients.
Dr. Mrudul Kyada, Department of Orthopedics, GMERS Medical College, Vadnagar, Gujarat, India. E-mail: mrudulkyada@ymail.com
Abstract
Introduction: Medial compartment osteoarthritis (OA) causes pain, functional limitation, and reduced quality of life. When conservative treatment fails, surgical options include high tibial osteotomy (HTO) and unicompartmental knee arthroplasty (UKA), both aimed at pain relief and functional improvement.
Materials and Methods: This prospective comparative study included 50 patients with isolated medial compartment OA, divided into UKA (n = 25) and HTO (n = 25) groups. Clinical parameters, including Visual Analogue Scale (VAS) pain score, ROM, and post-operative complications, were analysed, with P < 0.05 considered significant.
Results: Most patients were males (60%) and aged 50–70 years (76%). Pre-operative VAS scores were comparable (UKA: 7.8 ± 0.9; HTO: 7.6 ± 1.0). Post-operatively, pain significantly decreased in both groups but was lower in UKA (2.1 ± 0.8 vs. 3.2 ± 1.0; P = 0.01). Functional outcomes were better in the UKA group (knee society score: 86.4 ± 6.5 vs. 79.2 ± 7.3), with greater improvement in ROM (125° vs. 118°). Most patients (88%) had no complications.
Conclusion: Both HTO and UKA are effective for medial compartment OA; however, UKA provides superior functional outcomes and range of motion.
Keywords: Functional outcome, high tibial osteotomy, knee society score, medial compartment osteoarthritis, unicompartmental knee arthroplasty.
Knee osteoarthritis (OA) is a leading cause of disability, pain, and diminished quality of life among people globally. Inflammation of the synovia, remodellingg of the bone underneath the cartilage, development of osteophytes, and gradual loss of joint cartilage characterise this degenerative joint condition. Knee problems are common because the knee joint bears a disproportionate share of the body’s weight and experiences repetitive mechanical stress when performing common daily tasks, such as walking, stair climbing, and squatting. Since the lower leg is in a varus posture by nature, more weight is transmitted to the medial side of the knee, making it the most afflicted compartment of the knee joint. Patients with medial compartment OA have a lot of trouble moving about and doing everyday tasks since the condition is characterised by increasing pain, stiffness, deformity, and functional limitations [1,2]. The primary treatment for knee OA starts with conservative care methods. “The treatment programmeme requires people to change their daily habits and achieve weight loss while they complete their physical therapy sessions and use pain relief medication, non-steroidal anti-inflammatory drugs and joint injections of corticosteroids or hyaluronic acid. The treatments succeed in symptom reduction, but they do not prevent disease progression. Surgical procedures become necessary when a patient with chronic pain and functional impairment fails to respond to standard treatment methods. For younger patients who experience active medial compartment OA with preserved patellofemoral and lateral compartments, joint-preserving surgical methods may be preferable toomplete knee arthroplasty [3,4]. The ancient surgical procedure, high tibial osteotomy (HTO), operates as a medical treatment for varus deformity medial compartment OA. The primary goal of HTO is to realign the lower limb’s mechanical axis by shifting the lower limb’s weight-bearing axis to a more advantageous side of the lateral compartment. The HTO procedure uses weight distribution across the knee joint to decrease medial compartment stress, which provides pain relief while postponing OA progression. The method displays effective results for younger patients with high energy levels who want to boost their physical activity. Some research suggests that HTO may delay the need for complete knee replacement, improve functional capacity, and alleviate pain to a satisfactory degree. However, there is a longer recovery period involved, and problems, such as non-union, loss of correction, and irritation of hardware,, are possible [5,6]. Individuals suffering from medial compartment OA have an additional surgical option: Medial unicompartmental knee arthroplasty (UKA), sometimes known as partial knee replacement. When compared to HTO, which keeps the knee joint together and realigns the limbs, UKA is used to replace the damaged knee joint while preserving the healthy ligaments, bone, and cartilage in the others. In comparison to HTO, this procedure takes less time to recover from and produces faster pain relief by restoring normal joint kinematics. Patients undergoing UKA often report better functional outcomes, faster mobilisation, and increased range of motion (ROM). It is also easy to make revisions to a UKA if necessary in the future since less bone and soft tissue is removed compared to a total knee arthroplasty [7,8]. Medial UKA and high tibia osteotomy both have theirir advantages, but which one is better is still up for debate. There are indications, benefits, and limitations to every surgery. UKA may be recommended for elderly patients with local cartilage loss and generally stable ligaments, whereas HTO is often utilised for individuals with significant varus malalignment and high activity levels. There is, however, an ongoing debate about whether the procedure provides superior functional recovery, analgesia, and post-operative clinical outcomes due to the muddled symptoms and developments in surgical art [9,10]. Multiple studies have investigated the comparison between UKA and HTO outcomes for people who have isolated medial compartment OA. Research shows that UKA delivers quicker pain relief together with improved initial functional results, while HTO offers better joint preservation during the long term for younger patients. The various studies reached different conclusions because researchers employed different methods to select patients, conduct surgeries, and evaluate results [11,12]. The comparison of HTO functional and clinical outcomes with those of medial UKA must take place before surgical procedure selection. The advantages and disadvantages of various treatments for isolated medial compartment OA should be understood by professionals to determine the best treatment option for their patients. The study will evaluate functional outcomes and pain relief together with the clinical effectiveness of medial UKA combined with HTO for patients with isolated medial compartment OA. Despite the increasing use of both HTO and UKA for isolated medial compartment OA, there remains ongoing controversy regarding the optimal surgical procedure in terms of pain relief, functional recovery, ROM, and complication profile. Furthermore, limited prospective comparative data are available from the Indian population evaluating the clinical effectiveness of these procedures. Therefore, the present study was conducted to compare the functional and clinical outcomes of medial UKA and HTO in patients with isolated medial compartment OA of the knee.
Study design:
This study was designed as a prospective comparative observational study conducted to evaluate and compare the functional and clinical outcomes of medial UKA and HTO in patients with isolated medial compartment OA of the knee. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Study setting:
The study was conducted in the orthopaedics department of a tertiary care teaching hospital.
Study duration:
The study was carried out over a period of 18 months, including patient recruitment, surgical intervention, and post-operative follow-up.
Participants:
Patients diagnosed with isolated medial compartment OA of the knee, who presented to the orthopaedic outpatient department and were planned for surgical treatment, were considered for participation in the study.
Inclusion criteria:
- Patients aged between 40 and 70 years
- Patients diagnosed with isolated medial compartment OA of the knee, confirmed clinically and radiologically
- Patients with persistent knee pain and functional limitation despite conservative treatment
- Patients suitable for either medial UKA or HTO as determined by the orthopedic surgeon
- Patients who provided written informed consent to participate in the study.
Exclusion criteria:
- Patients with bicompartmental or tricompartmental OA of the knee
- Patients with inflammatory arthritis, such as rheumatoid arthritis
- Patients with previous knee surgery or fractures around the knee joint
- Patients with severe ligament instability of the knee
- Patients with severe systemic illness or contraindications to surgery
- Patients who were unwilling to participate or unable to comply with follow-up.
Study sampling:
A consecutive sampling technique was used in the study. The research staff selected study participants from all patients who visited the orthopaedic outpatient department during the study period while meeting the research requirements until they reached their target study sample size. The research study used this sampling approach to provide equal chances for all eligible patients to join the study who showed up at the research site during the study period.
Study sample size:
The sample size was calculated based on previous studies comparing functional outcomes between UKA and HTO groups, considering the post-operative knee society score (KSS) as the primary outcome variable. Assuming a confidence level of 95%, a power of 80%, and an expected mean difference (MD) between groups, the minimum required sample size was calculated to be 22 patients in each group. To account for possible loss to follow-up, 25 patients were included in each group, resulting in a total sample size of 50 patients.
Study groups:
The enrolled patients were divided into two groups based on the surgical procedure performed.
- Group A: Patients who underwent Medial UKA.
- Group B: Patients who underwent HTO.
Each group included 25 patients. Group allocation was performed based on clinical decision-making by the treating orthopaedic surgeon after evaluation of patient age, activity level, severity of varus deformity, radiological findings, cartilage status, and patient preference. Randomisation was not performed in the present study.
Study parameters:
The research examined both clinical results and functional results in patients who underwent two different surgical methods. The study measured the following parameters:
- Demographic variables, such as age, gender, and body mass index (BMI)
- The time period between the start of symptoms and the patient’s condition before surgery
- Pain intensity, assessed using the visual analog scale (VAS)
- The study measured functional results through standardized knee assessment tools, which included the KSS and Oxford Knee Score
- ROM of the knee joint measured using a goniometer
- Radiological assessment, including the degree of varus deformity and compartment involvement
- Post-operative complications, if any.
Study procedure:
Pre-operative clinical assessments for all patients included obtaining their medical history, doing a physical examination, and ordering imaging studies, such as lateral and weight-bearing anteroposteral and X-rays of the knee, to ensure a proper fit for the operation. Both UKA and HTO were to be administered to individuals who were determined to have isolated medial compartment OA and who met the eligibility criteria. The goal of medial UKA is to restore the patient’s knee joint’s healthy medial compartment while keeping the patient’s healthy lateral compartment, anterior cruciate ligament, and other bone structures. To alleviate pressure on the affected region, the patient who had had an HTO had to have the proximal tibia realigned during surgery so that the lower limb’s mechanical axis would be on the lateral side rather than the medial side. Following the procedure, all patients were given the standard care medications, including antibiotics, physiotherapy, and pain medication. It was encouraged to begin therapy and movement early to improve joint mobility and recovery.
Study data collection:
A pre-designed structured pro forma was used to collect data. Before the operation, demographic information, clinical results, and radiological parameters were documented. The follow-up evaluation was conducted periodically, where it was observed to record pain ratings, function results, range of movement, and complications. All the clinical data were captured in a systematic manner to make the data complete and accurate.
Data analysis:
The data obtained were put into Microsoft Excel and were analysed with the help of Statistical Package for the Social Sciences software. Demographic and clinical variables were summarised by using descriptive statistics, including mean, standard deviation, frequencies, and percentages. The two study groups were compared based on the relevant statistical tests, which included the use of an independent t-test in the examination of continuous variables and the chi-square test in the examination of categorical variables. The P < 0.05 was taken to be statistically significant.
A total of 50 patients with isolated medial compartment OA were included and equally divided into UKA (n = 25) and HTO (n = 25) groups. The majority of patients were in the 50–59 years and 60–70 years age groups (38% each). HTO was more commonly performed in relatively younger patients (40–59 years), whereas UKA was predominantly done in older patients (60–70 years), reflecting procedure selection based on age and activity level. Gender distribution showed a male predominance, with 30 males (60%) and 20 females (40%). A higher proportion of males underwent both procedures, particularly HTO, suggesting a greater burden of symptomatic medial compartment OA requiring surgery among male patients. Regarding BMI, most patients were overweight (46%), followed by normal BMI (28%) and obese (26%). Both groups had a similar BMI distribution, indicating that increased body weight is a significant contributing factor to the development of medial compartment OA. The duration of symptoms revealed that 48% of patients had symptoms for 1–3 years, 28% for more than 3 years, and 24% for <1 year. This suggests that most patients underwent surgery after prolonged symptom duration and failure of conservative management. Preoperatively, both groups had comparable pain levels, with mean VAS scores of 7.8 ± 0.9 in the UKA group and 7.6 ± 1.0 in the HTO group, indicating severe baseline pain. Post-operatively, both groups showed significant pain reduction; however, the UKA group demonstrated superior outcomes with a mean VAS score of 2.1 ± 0.8 compared to 3.2 ± 1.0 in the HTO group, which was statistically significant (P = 0.01). This indicates better early pain relief following UKA. Both groups showed significant improvement in functional outcome after surgery. The UKA group demonstrated higher post-operative KSS (86.4) compared to the HTO group (79.2), indicating better functional recovery following UKA (Table 1 and Fig. 1).
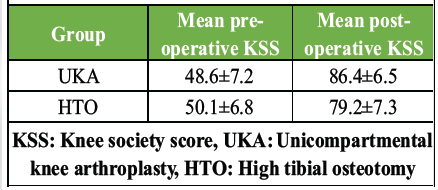
Table 1: Functional outcome based on KSS
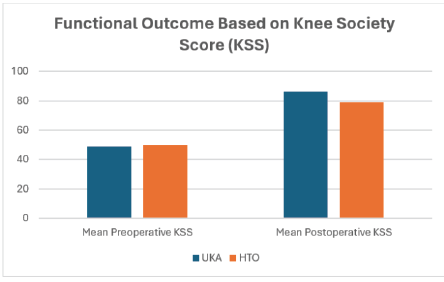
Figure 1: Functional outcome based on the Knee Society Score.
The ROM improved in both groups after surgery. However, the UKA group achieved a greater post-operative ROM (125°) compared to the HTO group (118°). This suggests that UKA may provide better post-operative knee mobility (Table 2 and Fig. 2).
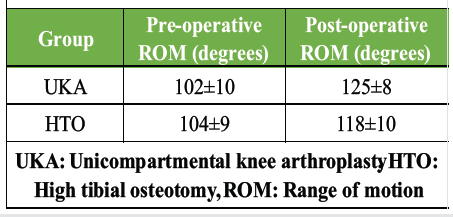
Table 2: Range of motion of knee joint
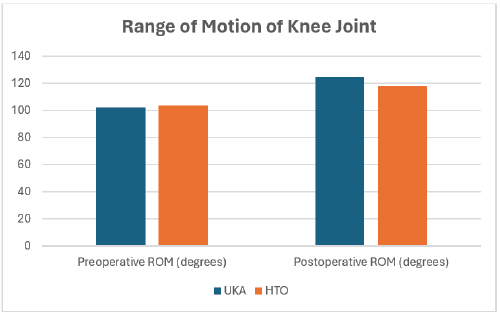
Figure 2: Range of motion of the knee joint.
Post-operative complications were minimal, with 44 patients (88%) experiencing no complications. Minor complications included infection in 3 patients (UKA: 1, HTO: 2), implant loosening in 1 patient (UKA), and delayed union in 2 patients (HTO). Delayed union was exclusive to the HTO group, while implant-related issues were observed only in the UKA group, indicating low and procedure-specific complication profiles (Table 3).
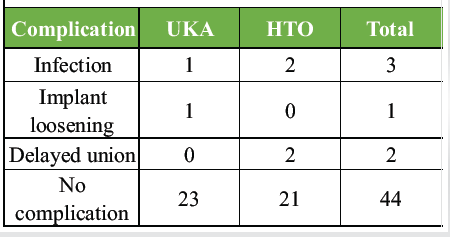
Table 3: Post-operative complications
In terms of functional outcomes, 80% of patients achieved good to excellent results, with 19 patients (38%) classified as excellent and 21 patients (42%) as good. The UKA group showed a higher proportion of excellent outcomes (12 vs. 7), whereas fair (3 vs. 5) and poor outcomes (0 vs. 2) were more common in the HTO group, suggesting comparatively better functional recovery with UKA.
This study aimed to assess the functional and clinical outcomes of two procedures for patients with isolated medial compartment OA of the knee: Medial UKA and HTO. We included 50 patients total; 25 of them received UKA and 25 received HTO. Topics included in the study were demographics, pain treatment, functional performance, ROM, complications, and overall results after surgery. The present research study finds its most beneficial application through the assessment of effectiveness between two surgical techniques for medial compartment OA treatment. The majority of patients, 50–60 years old, made up 38% of the total patient population in this study. HTO patients showed a younger age pattern since their median age reached 40–59 years, while UKA patients showed a 60–70-year age range. The research demonstrates that HTO treatment shows better results when doctors treat young active patients who need UKA than when doctors treat elderly patients with compartmentalized degeneration. With a mean age of 67.9 ± 9.0 years for the mobile bearing UKA group and 58.4 ± 5.5 years for the open-ended HTO group, Cho et al. [13] also found a comparable age difference between the two surgical groups, demonstrating that UKA is typically used in older patients with progressive medial OA. Among the patients surveyed for this research, 60% were men and 40% were female, according to the available data. Among these, 14 have had UKA performed on them, while 11 have had HTO done on them. A possible explanation for the somewhat higher incidence in men may be the increased mechanical stress on the knee joint caused by a wider variety of jobs. Even yet, there was little difference in the demographic make-up of the two categories. There was no statistically significant difference in age or BMI between patients who had HTO or UKA (P > 0.05) in the research by Cigercioglu et al. [14], demonstrating a similar equilibrium between the two groups. Blood pressure and BMI were also measured in this research. Overweight patients accounted for 46% of the total, whereas normal weight individuals made up 28%, and obese patients 26%. Twelve patients in the UKA group were overweight, compared to eleven in the HTO group. Overweight people are more likely to develop medial compartment OA, which puts extra stress on the knee joint, and the frequency of this condition is a testament to this. The average BMI in the HTO group was 30.93 ± 3.33 kg/m²,2 and in the UKA group it was 30.48 ± 3.57 kg/m²; this indicates that surgical intervention is often necessary for those who are overweight or obese to treat knee OA, as described by Cigercioglu et al. [14]. Symptom count before to surgery was also assessed in this research. Half of the patients had symptoms for 1–3 years, a quarter for <1 year, and a quarter for more than 3 years. The majority of patients had surgery after a protracted duration of symptoms and ineffectiveness of conservative treatments, according to these findings. This pattern is often seen in the OA literature, when surgical intervention is suggested as a solution after non-surgical methods of pain and functional limitation relief have been exhausted. When it comes to knee OA surgery, alleviating pain is one of the most important factors in determining a successful outcome. Results show that both the UKA and HTO groups had significant pain before surgery, with a pre-operative VAS score of 7.8, 0.9, and 7.6, 1.0, respectively. The VAS scores of the UKA and HTO groups declined to 2.1 + −0.8 and 3.2 + −1.0, respectively, after the surgeries because both treatments proved successful for pain relief. The UKA group, however, showed a statistically significant improvement (P = 0.01). Our results match those of another meta-analysis conducted by Han et al. [15], which showed UKA patients experienced reduced post-operative pain when compared to HTO patients (odds ratio [OR] 0.28, 95% confidence intervals [CI]: 0.12–0.62; P = 0.002). The study by Zhang et al. [16] found that UKA decreased post-operative pain while reducing complications at a statistically significant level because their P-value remained below 0.05. The research team used the KSS to evaluate functional outcomes of the study. The UKA group had an average pre-operative KSS score of 48.6 + 7.2, while the HTO group posted 50.1 + 6.8, which showed both groups had inadequate knee function before their operations. The UKA and HTO groups both achieved substantial functional enhancements after their surgical procedures, which resulted in their scores reaching 86.4 ± 6.5 and 79.2 ± 7.3. It seems that more joint functioning was restored following surgery, as the UKA group had a higher improvement after surgery. Results were comparable in a study by Nanda et al. [17], which found that after 24 months of follow-up, UKA had superior functional outcomes (40.1) compared to HTO (34.8) (P = 0.001). In addition, the functional scores, such as the Lysholm score (MD −2.78) and the Hospital for Special Surgery score (MD −2.80), were found to be considerably lower in the HTO group compared to the UKA group, as reported by Huang et al. [18]. The ROM of the knee joint is another important metric for assessing its functional status. Post-operative ROM increased from 102°C 10 before surgery in the UKA and 104°C 10 in the HTO, respectively, to 125°C 8 and 118°C 10 after the operation. There was an improvement in both groups; however, the UKA group had a little more advanced improvement. However, the results of ROM have been reported in a variety of ways. To provide an example, whereas Zhang et al. [16] proposed that HTO provided more mobility than UKA, Huang et al. [18] found no difference in post-operative ROM between HTO and mobile bearing UKA (MD −3.78, 95% CI −15.78 8.22). Of note, 44 patients (88%) in the present research did not have any problems after surgery. A few minor issues were infections in three patients, loose implants in one, and delayed union in two. The healing of the osteotomy was the only reason for the delayed union seen in the HTO group. As a consequence of a much higher complication rate in the HTO group (OR 4.88, 95% CI: 2.92686) compared to the UKA group, Huang et al. [18] also found comparable outcomes. The authors of the aforementioned study [15] also discovered that HTO significantly increased the risk of post-operative complications (OR 2.48, 95% CI: 1.264.90; P = 0.009). Finally, the present study’s overall functional outcomes showed that 12 patients in the UKA group had outstanding functional outcomes, compared to 7 patients in the HTO group. Meanwhile, 10 patients in the UKA group and 11 patients in the HTO group fared well. The only group that had shown any good outcomes was the HTO group. Despite the fact that both surgical procedures provide respectable clinical results, our findings indicate that UKA is more likely to achieve a larger proportion of good outcomes, measured by improved functional recovery and reduced discomfort. Similarly, Cho et al. [13] found that mobile-bearing UKA outperformed open-wedge HTO in terms of short-term clinical results, HSS improvements, and knee ratings. Both medial UKA and HTO have been reported in the literature as effective surgical treatments for isolated medial compartment OA; the present study’s findings corroborate these claims.” While HTO is a fantastic joint-preserving procedure, particularly for younger, more active patients, UKA has been shown to be superior in pain control, functional performance, and complication rates. Accordingly, it is advised that the correct surgical treatment be chosen on an individual basis based on patient age, activity level, deformity level, and expectations. The present study has several strengths. It was a prospective comparative study with uniform clinical assessment and standardised post-operative evaluation of both surgical procedures. Multiple outcome parameters, including pain score, functional outcome, ROM, and complications, were evaluated, allowing comprehensive comparison between UKA and HTO. However, the study also has certain limitations. The sample size was relatively small, and the follow-up duration was short, limiting assessment of long-term implant survival and disease progression. The study was conducted at a single centre, which may limit the generalisability of the findings. In addition, randomisation was not performed, which may introduce selection bias during the allocation of surgical procedures. Further multicentric studies with a larger sample size and longer follow-up are recommended for more definitive conclusions.
Both medial UKA and HTO are effective surgical options for isolated medial compartment OA of the knee. However, UKA demonstrated comparatively better functional recovery, pain relief, and post-operative knee mobility. HTO remains a valuable joint-preserving procedure, particularly in younger and physically active individuals. Appropriate procedure selection should be individualized according to patient characteristics, deformity, activity level, and surgeon expertise.
Both UKA and HTO are effective for isolated medial compartment osteoarthritis, but UKA provides superior short-term pain relief, function, and range of motion. HTO remains a valuable joint-preserving option in younger, active patients, and procedure selection should be individualized based on patient profile and surgeon expertise.
References
- 1. Smith WB 2nd, Steinberg J, Scholtes S, Mcnamara IR. Medial compartment knee osteoarthritis: Age-stratified cost-effectiveness of total knee arthroplasty, unicompartmental knee arthroplasty, and high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2017;25:924-33. [Google Scholar] [PubMed]
- 2. Ledingham J, Regan M, Jones A, Doherty M. Radiographic patterns and associations of osteoarthritis of the knee in patients referred to hospital. Ann Rheum Dis 1993;52:520-6. [Google Scholar] [PubMed]
- 3. Wise BL, Niu J, Yang M, Lane NE, Harvey W, Felson DT, et al. Patterns of compartment involvement in tibiofemoral osteoarthritis in men and women and in whites and African Americans. Arthritis Care Res 2012;64:847-52. [Google Scholar] [PubMed]
- 4. Chen G, Xu B, Xie J, Nie Y, Tang S, Ma J, et al. Comparison of clinical and biomechanical outcomes between partial fibulectomy and drug conservative treatment for medial knee osteoarthritis. Biomed Res Int 2019;2019:4575424. [Google Scholar] [PubMed]
- 5. D’Ambrosi R, Da Silva M, Moura JL, Mariani I, Serrao LD, Di Feo F, et al. Radiographic and clinical evolution of the oxford unicompartmental knee arthroplasty. J Knee Surg 2023;36:246-53. [Google Scholar] [PubMed]
- 6. Ji W, Luo C, Zhan Y, Xie X, He Q, Zhang B. A residual intra-articular varus after medial opening wedge high tibial osteotomy (HTO) for varus osteoarthritis of the knee. Arch Orthop Trauma Surg 2019;139:743-50. [Google Scholar] [PubMed]
- 7. D’Ambrosi R, Buda M, Nuara A, Mariani I, Scelsi M, Valli F, et al. Patellar height after unicompartmental knee arthroplasty: Comparison between fixed and mobile bearing. Arch Orthop Trauma Surg 2022;142:3449-60. [Google Scholar] [PubMed]
- 8. Tuhanioglu U, Ogur HU, Seyfettinoglu F, Çiçek H, Gültekin A. High tibial osteotomy in obese patients: Is successful surgery enough for a good outcome? J Clin Orthop Trauma 2019;10 Suppl 1:S168-73. [Google Scholar] [PubMed]
- 9. Jin QH, Lee WG, Song EK, Jin C, Seon JK. Comparison of long-term survival analysis between open-wedge high tibial osteotomy and unicompartmental knee arthroplasty. J Arthroplasty 2021;36:1562-7. [Google Scholar] [PubMed]
- 10. Maxwell R, Johnston A, Lees D, Walker C. Knee OUTcome study: A comparison of the patient perceived outcome between high tibial osteotomy, unicompartmental and total knee arthroplasty for medial compartment osteoarthitis in men under age 55. Orthop J Sports Med 2017;5 Suppl 5:2325967117S2325960016. [Google Scholar] [PubMed]
- 11. Yim JH, Song EK, Seo HY, Kim MS, Seon JK. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty at a minimum follow-up of 3 years. J Arthroplasty 2013;28:243-7. [Google Scholar] [PubMed]
- 12. Akizuki S, Shibakawa A, Takizawa T, Yamazaki I, Horiuchi H. The long-term outcome of high tibial osteotomy: A ten- to 20-year follow-up. J Bone Joint Surg Br Vol 2008;90:592-6. [Google Scholar] [PubMed]
- 13. Cho WJ, Kim JM, Kim WK, Kim DE, Kim NK, Bin SI. Mobile-bearing unicompartmental knee arthroplasty in old-aged patients demonstrates superior short-term clinical outcomes to open-wedge high tibial osteotomy in middle-aged patients with advanced isolated medial osteoarthritis. Int Orthop 2018;42:2357-63. [Google Scholar] [PubMed]
- 14. Cigercioglu N, Ozer H, Baltaci G. Comparison of functional outcomes of high tibial osteotomy and unicompartmental knee arthroplasty in patients with medial knee osteoarthritis. J Knee Surg 2025;39:195-9. [Google Scholar] [PubMed]
- 15. Han SB, Kyung HS, Seo IW, Shin YS. Better clinical outcomes after unicompartmental knee arthroplasty when comparing with high tibial osteotomy. Medicine (Baltimore) 2017;96:e9268. [Google Scholar] [PubMed]
- 16. Zhang B, Qian H, Wu H, Yang X. Unicompartmental knee arthroplasty versus high tibial osteotomy for medial knee osteoarthritis: A systematic review and meta-analysis. J Orthop Surg (Hong Hong) 2023;31:10225536231162829. [Google Scholar] [PubMed]
- 17. Nanda SN, Gachhayat A, Kaushik S, Mishra D, Tyagi A, Poddar S. Medial unicompartmental knee arthroplasty vs. High tibial osteotomy for isolated medial knee osteoarthritis: A propensity-matched study of clinical outcomes. Indian J Orthop 2025;60:458-64. [Google Scholar] [PubMed]
- 18. Huang L, Xu Y, Wei L, Yuan G, Chen W, Gao S, et al. Unicompartmental knee arthroplasty is superior to high tibial osteotomy for the treatment of medial unicompartmental osteoarthritis: A systematic review and meta-analysis. Medicine (Baltimore) 2022;101:e29576. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 September 10, 2020 An Extremely Rare Combination of Monteggia Equivalent Type 1 Lesion (diaphyseal Ulna and Radial Neck Fractures Without Dislocation) with Ipsilateral Radius Shaft and Distal Radius Fractures in a Child
September 10, 2020 An Extremely Rare Combination of Monteggia Equivalent Type 1 Lesion (diaphyseal Ulna and Radial Neck Fractures Without Dislocation) with Ipsilateral Radius Shaft and Distal Radius Fractures in a Child October 10, 2020 Osteosynthesis in Neglected Femoral Neck Fracture in an Adolescent by Internal Fixation Alone – A Case Report
October 10, 2020 Osteosynthesis in Neglected Femoral Neck Fracture in an Adolescent by Internal Fixation Alone – A Case Report March 1, 2025 Myxoma of the Dorsal Aspect of the Hand – A Case Report of a Rare Condition
March 1, 2025 Myxoma of the Dorsal Aspect of the Hand – A Case Report of a Rare Condition April 1, 2025 A Revision of an Infected Total Hip Arthroplasty leading to Oxalate Nephropathy: A Case Report
April 1, 2025 A Revision of an Infected Total Hip Arthroplasty leading to Oxalate Nephropathy: A Case Report