
Although technically demanding, arthroplasty can achieve meaningful pain relief and improved quality of life in carefully selected post-poliomyelitis patients.
Dr. Dliyauddin Fachri, Department of Orthopaedics and Traumatology Faculty of Medicine Padjadjaran University/Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia. E-mail: aifachri690@gmail.com
Abstract
Introduction: Patients with poliomyelitis can have long-term sequelae such as paralysis and muscle weakness in their lower limbs caused by motor atrophy and degradation of motor and autonomic neurones. Patients can also develop osteoporosis, causing instability. This leads to a greater risk of falls and fractures, such as hip fractures. There are difficulties and risks in doing management, especially doing total hip arthroplasty (THA) in polio patients due to differences in anatomy and function of the lower limb.
Case Report: A 70-year-old woman came to the hospital with pain in her left hip after she slipped and landed on her left hip 5 h before. She underwent femoral surgery 30 years ago and has a history of polio. She was diagnosed with a periprosthetic fracture at the left femoral neck post-open reduction and internal fixation with a plate and screws with equinus deformity at the left ankle due to poliomyelitis and osteopenia. She then undergoes implant removal and total hip replacement with cerclage wire. The surgery showed excellent results, with no sign of infection or dislocation and significant pain improvement. Further physiotherapy will lead to an improvement in motoric function.
Conclusion: THA in patients with poliomyelitis presents with several complications and difficulties. However, if the indication outweighs the risk, it should be done with good surgical planning and close post-operative follow-up and rehabilitation
Keywords: Total hip arthroplasty, poliomyelitis, femoral neck fracture, equinus deformity.
Poliomyelitis is a disease infecting the anterior horn cell of the spinal cord, affecting motor function [1]. Polio is so close to being eradicated after the invention of the polio vaccine. To this day, there are still patients living with the long-term sequelae of polio even years after the last epidemic of poliomyelitis [2]. These patients mostly live in developing nations or have economic disadvantages. Recovery may be worse in patients with loss of motor function beyond 12 months [3]. Polio can cause degradation of motor and autonomic neurones, leading to paralysis and muscle weakness [2,4]. Abnormal gait patterns and motor impairment caused by muscular atrophy and leg weakness are some of the reasons for a greater risk of falls in poliomyelitis patients [5]. These complaints are most commonly experienced in the lower limb because the virus often targets the anterior horn cells of L2 and L3 that innervate the quadriceps [6]. Adults with polio are also more likely to have low bone mass, causing osteoporosis [5]. Recent investigations showed that there are risks for patients with polio to develop degenerative hip arthritis, which leads to instability [2]. These risks can lead to fractures. These conditions are called post-polio syndrome, in which symptoms of paresis and paralysis of polio can return many decades after the original infection [6]. These complaints will worsen as the patients age due to degenerative changes [7]. The great risk of falls and fractures in poliomyelitis patients may lead to the patients needing total arthroplasty, such as total hip arthroplasty (THA), especially after a fracture. Proximal fractures are among the most common osteoporotic fractures and can cause further motoric and gait issues [8]. However, there is still a small number of published literature discussions about the management of femoral fracture and the effect of THA in poliomyelitis patients because, although replacement surgery is the most common treatment for the “normal” patients, poliomyelitis patients have anatomical and physiological differences causing difficulty and risk of complication. This report presents a case of a poliomyelitis patient with a periprosthetic fracture at the left femoral neck post-open reduction and internal fixation (ORIF) plate and screws and osteopenia who then underwent successful THA with cerclage wire and continued with a boot cast for immobilisation and lengthening of the Achilles tendon. Despite the risk and difficulty, we hope this case report can highlight the possibility and outcome of THA in poliomyelitis patients.
A 70-year-old woman came to the hospital with pain in her left hip after she slipped and landed on her left hip 5 h before. After the incident, the patient complained of pain in the left hip but could still bear her body weight, with no complaints about other body parts. She underwent femoral surgery 30 years ago and has a history of polio. Before the fall, the patient used a walker in her day-to-day life. She denied taking any medicine or doing any intervention before coming to the hospital. When examined, shortening and muscle wasting in her left thigh and leg with tenderness limited her range of movement (Fig. 1).

Figure 1: Pre-operative patient presentation.
The apparent length of her right leg is 88 cm, while her left leg is 86 cm, and the true length was 79 cm and 77 cm for her right and left legs, respectively. There was also equinus deformity in her left knee. The X-ray showed bone discontinuity at the left neck femur without implant failure. Bone mineral density results showed osteopenia in vertebrae with a T score of −0.9 standard deviation (SD) and a Z score of 1.3 SD; the right femur with a T score of −1.8 SD and a Z score of −0.3 SD; and the right forearm with a T score of −1.8 SD and a Z score of −0.3 SD (Fig. 2).
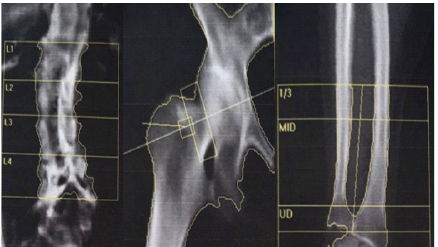
Figure 2: Bone mineral density result in L1-L4 vertebrae, right hip, and right forearm showing osteopenia.
The ultrasound Doppler of the lower extremity showed no plaque, and there was good flow in both arteries, and a 3D reconstruction was made (Fig. 3).
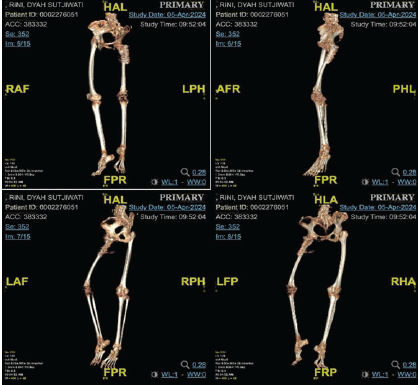
Figure 3: 3D bone reconstruction from magnetic resonance imaging.
There was no thrombus in the vein or chronic venous insufficiency. She was diagnosed with a periprosthetic fracture at the left femoral neck post-ORIF plate and screws with equinus deformity at the left ankle due to poliomyelitis and osteopenia (Figs. 4, 5, and 6).
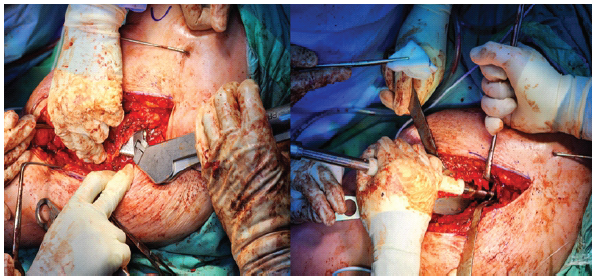
Figure 4: Intraoperative reaming of femur and acetabular.
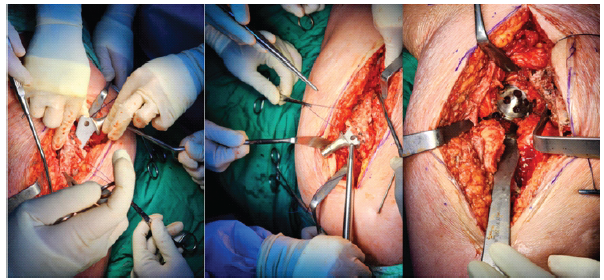
Figure 5: Intraoperative insertion of femoral stem and acetabular cup.
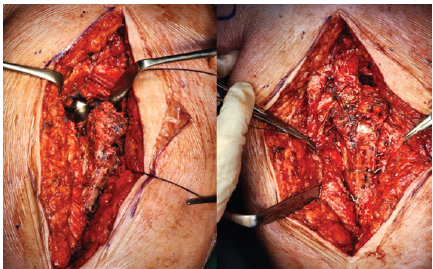
Figure 6: Intraoperative post-implant and cerclage wire insertion.
A surgical intervention was required, so implant removal and total hip replacement with cerclage wire were performed. The patient was in the lateral position with a direct lateral approach for implant removal and total hip replacement. After that, she wears a boot cast for immobilisation after Achilles tendon lengthening (Fig. 7).
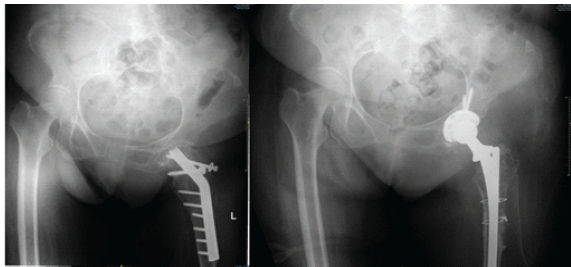
Figure 7: Post-operative imaging showing neglected femoral neck fracture post-open reduction and internal fixation with plate and screw, and post-operative imaging showing post-total hip replacement and cerclage wire.
Five days post-surgery, the patient showed excellent results, with less tenderness in the left hip and no sign of infection, such as swelling, pus, fever, or leukocytosis. Her range of movement is still limited due to pain. The lab results from 4 days post-surgery were 9.5 g/dL in haemoglobin, 28.4% in haematocrit, 7010 in leukocyte, and 204,000 in thrombocyte. The patient was then discharged with a future rehabilitation plan to increase range of movement with physiotherapy and instructed not to bear weight on the fractured limb (Fig. 8). At the the 2-year follow-up, the patient was pain-free and able to walk with crutches (Fig. 9).

Figure 8: Five days post-surgery, showing the patient was able to sit down without support and still wearing boot cast for immobilization after lengthening of achilles tendon.

Figure 9: At 2 years follow-up, showing that the patient was pain-free and able to walk with crutches.
There are a significant number of complications that can happen to poliomyelitis patients after THA surgery, such as dislocation, non-unions, peri-implant fractures, malunion, cutout, and prominent hardware, which can lead to re-operation, causing many surgeons to feel reluctant to do it [8,9,10]. Some difficulties can affect the surgery due to the pathological difference in anatomy and function in patients with poliomyelitis, such as weakening bone due to osteoporosis, deformity in bone size and structure, sequelae from previous fractures or surgery, weakening of the abductor muscle, and a narrow intramedullary canal [9,11]. These factors cause most poliomyelitis patients with fractures to undergo conservative treatment, unlike other cases where the main treatments are surgical and aggressive rehabilitation. Rehabilitation in poliomyelitis patients can also be troubled by low bone mass, low muscle strength, and impaired gait [8]. This case highlights the significant impact of poliomyelitis on bone health, particularly in the context of trauma and surgical intervention. Polio survivors are at an increased risk for osteoporosis, with studies showing that up to 96% of polio patients exhibit osteopenia or osteoporosis, making them highly susceptible to fractures [12]. In this patient, her history of polio combined with advanced age likely contributed to her osteopenic condition, which predisposed her to a periprosthetic fracture after a fall. In addition, recurrent falls are common in post-polio patients, with 39.2% experiencing falls and a subsequent higher incidence of fractures [13]. This combination of poor bone density and fall risk underscores the challenges faced by clinicians managing similar cases. Bone healing in polio-affected patients is often compromised due to reduced vascularity, disuse atrophy, and poor bone stock. The asymmetrical bone loss commonly observed in these patients further complicates recovery after surgeries like arthroplasty or fracture fixation [14]. In this case, the patient’s pre-existing equinus deformity at the left ankle – likely a sequela of poliomyelitis – indicates long-standing musculoskeletal abnormalities that may have contributed to altered biomechanics and stress distribution across the hip joint. In pre-operative assessment, poor bone quality, such as a narrow canal and osteoporosis, is commonly found with acetabular dysplasia in polio patients. These conditions, combined with weakened hip abductors, can lead to difficulty achieving stability of the acetabular component and lead to periprosthetic intraoperative fracture [9]. Our patient had osteopenia in her vertebrae, femur, and forearm, combined with a past fracture and surgery and weakened muscle, proven by abnormal gait and the need to use a walker to walk. These conditions showed that our patient has the risk of complications and difficulty. Data from recent publications show that fall rates in poliomyelitis patients are 66–74%, and up to 35% of these patients have a history of previous fractures from a fall [9]. A cohort study showed that adults with poliomyelitis have a higher risk of femoral neck or hip fractures than other adults [5,8]. This can be caused by muscle paralysis in polio due to quadriceps weakness, imbalanced gait due to deformities, contractures, or limb length discrepancies [11]. This also happened to our patient, who had a neck femoral fracture resulting from a fall, and this was not her first femoral fracture. The most common treatment for those patients was conservative, considering it is safer; meanwhile, the risk and difficulty of surgical intervention may outweigh the benefit. Conservative management was not pursued in this acute setting due to the severity of the periprosthetic fracture; it remains a viable option for less severe injuries or as part of post-operative care. Non-operative approaches, such as pharmacotherapy with bisphosphonates, can improve femoral neck bone mineral density in post-polio patients, potentially reducing future fracture risks [15]. Physical therapy focused on strengthening unaffected muscles and improving balance could help mitigate fall risks, with tailored rehabilitation emphasising gait training and mobility enhancement being particularly essential given the patient’s equinus deformity and prior surgery. In addition, assistive devices like braces or walking aids may help offload stress from fragile bones and joints, preventing further damage [12]. However, in this specific case, conservative measures alone would have been insufficient to address the periprosthetic fracture, making surgical intervention necessary. Several publications have shown that many THAs done to poliomyelitis patients did not show dislocation episodes or significant complications [6]. The average Harris score also showed improvement and decreased VAS score postoperatively [10]. They also showed improvement in functional and radiographic parameters [2]. Surgical treatment of fractures of the lower limbs in patients with poliomyelitis is possible. It can be done when the benefits outweigh the risks as long as there is good surgical planning and anticipation for possible intraoperative problems followed by postoperative rehabilitation [6,9]. For patients with advanced and painful degenerative changes and fractures, THA is the best option because if left untreated or using conservative treatments, it could lead to damaging the previously normal contralateral hip because of increasing load or further severe deformities of the affected hip, such as discrepancy in leg length, causing greater instability and fall risk [10]. Patients with femoral neck or hip fracture have a risk of dying within 1 year, and even then, more than half of those patients have difficulty walking, compromising their quality of life [5]. Meanwhile, conservative treatment has its risks, such as malunion, contractures, and pressure sores. In the long run, conservative treatment, if it is not adequate to the injury and degenerative changes, could predispose to further mobility problems, leading to loss of muscle mass and strength and osteoporosis [11]. In doing THA, long, slim stems and a restrictive or dual mobility acetabular system are recommended [9]. While post-operative complications still exist, they occur 2 years after surgery and can be fixed with surgical fixation of periprosthetic fractures. Modern implants have lessened the number of reoperations and revisions needed in the patients [2]. In evaluating the optimal treatment strategy for peri-implant fractures in patients with polio sequelae, a literature review (Table 1) underscores the importance of a multifaceted surgical approach.
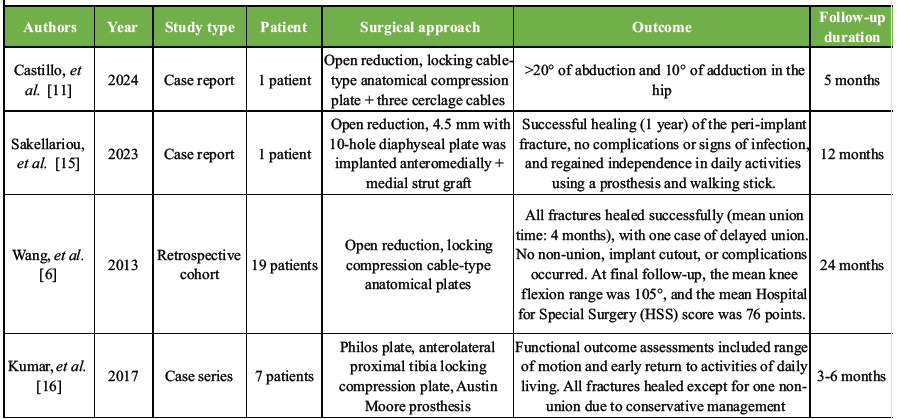
Table 1: A comprehensive review of the existing literature and available manuscripts
Advanced fixation techniques, such as those involving locking plates and cables, have demonstrated significant improvements in joint function and mobility, as evidenced by successful case reports and cohort studies [16,17]. These methods not only promote robust bone healing but also enhance functional recovery, enabling patients to regain independence in daily activities. However, conservative management approaches have been associated with higher rates of non-union and complications, highlighting the critical need for early surgical intervention. Given the high mortality rates observed post-fracture, a proactive and integrated treatment strategy becomes imperative [18,19]. This approach should combine open reduction with stable internal fixation using advanced locking plates and cables, complemented by diligent post-operative rehabilitation. Such a strategy not only mitigates the risk of complications but also fosters expedient functional recovery, ultimately enhancing the overall quality of life for this vulnerable patient population [16,17,18,19]. Initially, the patient underwent ORIF with plates and screws following her femoral surgery 30 years ago. However, plate fixation in polio patients carries inherent risks, including hardware failure due to poor bone stock, which increases the likelihood of screw pullout or plate breakage, as well as delayed union or non-union caused by impaired vascularity and osteoporosis that hinder proper bone healing [20]. In addition, polio-related soft-tissue atrophy and scar formation elevate the risk of post-surgical infections. In contrast, the decision to perform implant removal and proceed with THR (total hip replacement) using cerclage wires proved advantageous in this scenario. THR offers superior long-term outcomes for periprosthetic fractures in elderly patients with osteopenia, providing better stability and pain relief compared to revision ORIF [21]. The absence of post-operative complications, such as infection or dislocation, further highlights the efficacy of this approach when tailored to the patient’s unique anatomical and physiological challenges. Several factors contributed to the successful outcome of this patient’s treatment. Pre-operative imaging likely revealed significant osteopenia, guiding the decision to pursue THR over alternative methods like plate fixation. Given the patient’s age, functional limitations, and history of polio, restoring mobility and alleviating pain were prioritised, with THR aligning well with these goals. Collaboration between orthopaedic surgeons, physical therapists, and rehabilitation specialists ensured comprehensive care tailored to the patient’s unique condition. While the surgery yielded excellent results, ongoing physiotherapy will be critical in maximising motor function and preventing future falls, emphasising the importance of realistic expectations and continued multidisciplinary support for long-term success. The patient underwent implant removal followed by THA with the use of cerclage wires, along with postoperative immobilisation using a boot cast and Achilles tendon lengthening. These interventions were selected based on several indications for THA, primarily the presence of a femoral neck fracture causing significant pain and deformity. In addition, the patient exhibited degenerative changes, including osteopenia and leg length discrepancy, which further supported the decision for THA. The surgical procedure was successfully performed without any notable complications, yielding excellent outcomes. Postoperatively, the patient experienced significant pain reduction, and motor function demonstrated substantial potential for improvement, provided that rehabilitation was continued as planned. This case underscores that THA can be a viable option in poliomyelitis patients when clinically indicated and appropriately tailored to the individual’s condition.
The following case highlights the challenges of managing fractures in polio patients, who are at increased risk of osteoporosis, falls, and complications due to weakened bones, muscles, and altered biomechanics. While conservative treatment is often preferred in less severe cases, surgical intervention was necessary here to address the fracture and improve mobility. THR proved effective, providing stability and pain relief without post-operative complications, underscoring its viability for such complex cases when tailored to the patient’s unique condition. Successful outcomes were achieved through meticulous surgical planning, multidisciplinary care, and a structured rehabilitation plan aimed at restoring function and preventing future falls.
Careful preoperative assessment of muscle strength, joint stability, limb alignment, and functional expectations is essential to optimize surgical planning and outcomes. Despite technical difficulties, arthroplasty can provide substantial pain relief and functional improvement in selected post-poliomyelitis patients.
References
- 1. Chu EC, Lam KK. Post-poliomyelitis syndrome. Int Med Case Rep J 2019;12:261-4. [Google Scholar] [PubMed]
- 2. Dedeugd CM, Perry KI, Trousdale WH, Taunton MJ, Lewallen DG, Abdel MP, et al. Total hip arthroplasty in patients affected by poliomyelitis. Bone Joint J 2018;100-B:733-9. [Google Scholar] [PubMed]
- 3. Mehndiratta MM, Mehndiratta P, Pande R. Poliomyelitis: Historical facts, epidemiology, and current challenges in eradication. Neurohospitalist 2014;4:223-9. [Google Scholar] [PubMed]
- 4. Tigani D, Fosco M, Amendola L, Boriani L. Total knee arthroplasty in patients with poliomyelitis. Knee 2009;16:501-6. [Google Scholar] [PubMed]
- 5. Wu CH, Huang SW, Lin YN, Wang CY, Liou TH, Chang KH. Adults with polio are at risk of hip fracture from middle age: A nationwide population-based cohort study. Injury 2019;50:738-43. [Google Scholar] [PubMed]
- 6. Akadiri M, Smith C, Wong F, Davidson J. Total hip arthroplasties in polio survivors: A systematic review. J Hip Surg 2023;7:126-32. [Google Scholar] [PubMed]
- 7. Bickerstaffe A, Beelen A, Nollet F. Circumstances and consequences of falls in polio survivors. J Rehabil Med 2010;42:908-15. [Google Scholar] [PubMed]
- 8. Gellman YN, Khoury A, Liebergall M, Mosheiff R, Weil YA. Outcome of femoral fractures in poliomyelitis patients. Int Orthop 2019;43:2607-12. [Google Scholar] [PubMed]
- 9. Mingo-Robinet J, Alonso JA, Moreno-Barrero M, González-García L, Garcia-Virto V, Aguado HJ. Technical aspects and complications in the surgical treatment of poliomyelitis-affected lower limb fractures. Rev Esp Cir Ortop Traumatol (Engl Ed) 2018;62:257-66. [Google Scholar] [PubMed]
- 10. Yoon BH, Lee YK, Yoo JJ, Kim HJ, Koo KH. Total hip arthroplasty performed in patients with residual poliomyelitis: Does it work? Clin Orthop Relat Res 2014;472:933-40. [Google Scholar] [PubMed]
- 11. Gupta M, Jain VK, Upadhyaya GK, Arya RK. Comprehensive review of challenges associated with management of lower limb fractures in poliomyelitis patients. J Clin Orthop Trauma 2016;7:276-81. [Google Scholar] [PubMed]
- 12. Mohammad AF, Khan KA, Galvin L, Hardiman O, O’Connell PG. High incidence of osteoporosis and fractures in an aging post-polio population. Eur Neurol 2009;62:369-74. [Google Scholar] [PubMed]
- 13. Sherf RM, Cantrell D, Or K, Marcus E, Shapira A, Benbassat C, et al. The risk of bone fractures in post-poliomyelitis patients transitioning to middle adulthood. Endocr Pract 2020;26:1277-85. [Google Scholar] [PubMed]
- 14. Kushchayeva Y, Pestun I, Kushchayev S, Radzikhovska N, Lewiecki EM. Advancement in the treatment of osteoporosis and the effects on bone healing. J Clin Med 2022;11:7477. [Google Scholar] [PubMed]
- 15. Alvarez A, Kremer R, Weiss DR, Benedetti A, Haziza M, Trojan DA. Response of postpoliomyelitis patients to bisphosphonate treatment. PM R 2010;2:1094-103. [Google Scholar] [PubMed]
- 16. Padilla-Del Castillo KN, Rivas-Meléndez R, Méndez-Ortiz JA, Miramontes-Hernández AS, Robledo-González JL. Fractura periprotésica en un paciente con secuelas de polio: Reporte de caso. Salud Jalisco 2024;11:27-31. [Google Scholar] [PubMed]
- 17. Sakellariou E, Galanis A, Vavourakis M, Papagrigorakis E, Vlachos C, Zachariou D, et al. Peri-implant proximal femur fracture in a poliomyelitis survivor: A surgical and medical challenge. Clin Case Rep 2023;11:e7465. [Google Scholar] [PubMed]
- 18. Wang WJ, Shi HF, Chen DY, Chen YX, Wang JF, Wang SF, et al. Distal femoral fractures in post-poliomyelitis patients treated with locking compression plates. Orthop Surg 2013;5:118-23. [Google Scholar] [PubMed]
- 19. Kumar TS, Senthilnathan A, Prabhakar R. Choice of implants in management of fractures in patients with post-polio residual paralysis. Int J Orthop Sci 2017;3:577-83. [Google Scholar] [PubMed]
- 20. El-Sayed Khalil A. Locked plating for femoral fractures in polio patients. Arch Orthop Trauma Surg 2010;130:1299-304. [Google Scholar] [PubMed]
- 21. Capone A, Congia S, Civinini R, Marongiu G. Periprosthetic fractures: Epidemiology and current treatment. Clin Cases Miner Bone Metab 2017;14:189-96. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Outcomes of Total Hip Arthroplasty for Traumatic versus Non-Traumatic Hip Pathology: A Prospective Cohort Study
April 1, 2026 Outcomes of Total Hip Arthroplasty for Traumatic versus Non-Traumatic Hip Pathology: A Prospective Cohort Study August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report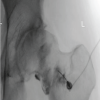 August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections