
Traumatic asymmetric bilateral shoulder dislocation is an extremely rare injury pattern that requires a high index of suspicion and careful radiological assessment to avoid a missed diagnosis, particularly of posterior shoulder dislocation.
Dr. Jesus David Gonzalez Valdovinos, Department of Trauma and Orthopedics, Hospital Central Norte of Petróleos Mexicanos, Mexico City, Mexico. E-mail: davidgonzalesvaldovinos@gmail.com
Abstract
Introduction: Asymmetric bilateral shoulder dislocation is an exceptionally rare pattern of glenohumeral injury characterised by simultaneous dislocation of both shoulders in different directions. Since its first description in 1985, only a limited number of cases have been reported worldwide. Most cases are associated with seizures or electrical injuries, while traumatic mechanisms are uncommon. Reporting additional cases is important to improve recognition and management of this unusual injury pattern.
Case Report: We report the case of a 39-year-old Hispanic male who presented to the emergency department after a high-energy motorcycle accident. Clinical examination revealed bilateral shoulder deformity and severe pain with marked limitation of motion, without neurovascular deficits. Radiographic evaluation demonstrated asymmetric bilateral glenohumeral dislocation, consisting of an anterior subglenoid dislocation of the left shoulder and a posterior dislocation of the right shoulder. Computed tomography confirmed a non-engaging reverse Hill–Sachs lesion involving approximately 18% of the articular surface of the right humeral head. Urgent closed reduction under sedation was successfully performed using different reduction manoeuvres for each shoulder, achieving stable joint congruency. The patient was managed conservatively with temporary immobilisation followed by progressive physical rehabilitation. During follow-up, the patient demonstrated progressive improvement in pain and range of motion. At 6 months, full functional recovery was achieved without recurrence or complications.
Conclusion: This report describes the first documented case in Mexico of traumatic asymmetric bilateral shoulder dislocation caused by a high-energy mechanism without associated fractures. The case highlights the importance of maintaining a high index of suspicion and performing a comprehensive radiological evaluation in patients with shoulder trauma. Early diagnosis and prompt closed reduction followed by appropriate rehabilitation can lead to favourable functional outcomes even in rare and complex injury patterns.
Keywords: Shoulder dislocation, joint dislocations, shoulder injuries, motorcycle accidents, case reports.
Shoulder dislocations are among the most common joint injuries in adults and account for approximately 50% of all peripheral dislocations. Anterior dislocation is by far the most frequent type, with a reported incidence ranging from 95% to 97% of cases, followed by posterior dislocation (2–4%) and inferior dislocation, which occurs in <1% of patients [1,2]. Within this spectrum, asymmetric bilateral shoulder dislocations, defined as the simultaneous dislocation of both glenohumeral joints in different directions (anterior, posterior, or inferior), represent an exceptionally rare entity. Since the first case described by Aufderheide et al. in 1985 [3], only ten additional reports have subsequently been published in international literature [4-13]. Analysis of the published cases shows that most of these injuries occur in male patients with a wide age range and are primarily associated with seizure episodes. Less frequently, they are related to low-energy trauma, electrical injuries, or combined mechanisms [3,4,5,6,7,8,9,10,11,12,13]. Regarding the injury pattern, the most reported combination is anterior–posterior (opposite-direction pattern), although variants involving inferior dislocation or chronic presentations have also been described [4,5,6,7,13]. In addition, most reported cases are associated with fractures of the proximal humerus, glenoid rim injuries, or other osseous defects, which increases diagnostic and therapeutic complexity [6, 8-12]. The diagnosis is mainly based on clinical evaluation and imaging studies. Radiography remains the initial diagnostic modality of choice and is often complemented by computed tomography to characterise associated bone injuries and guide therapeutic decision-making [5,6,7,8,9,10,11,12,13]. Management strategies reported in the literature are heterogeneous and range from closed reduction with conservative treatment to complex surgical procedures, depending on joint stability, associated injuries, and the patient’s functional status. In this context, we present the first documented case in Mexico of traumatic asymmetric bilateral shoulder dislocation, successfully treated with conservative management and objective functional evaluation using the Disabilities of the Arm, Shoulder, and Hand (DASH) score, contributing additional clinical evidence to this extremely rare condition.
A 39-year-old male patient with no relevant past medical history presented to the emergency department following a motorcycle accident. The patient was travelling as a passenger without a protective helmet at an approximate speed of 50 km/h when the driver performed a sudden brake manoeuvre, causing the patient to be projected approximately two metres and impact the pavement directly on both shoulders and the head. No warning signs of traumatic brain injury or loss of consciousness were documented. On physical examination, the patient presented with severe bilateral shoulder pain, loss of the normal rounded contour of both shoulders, and marked limitation of both active and passive range of motion. No neurological deficits or distal vascular compromise was identified in the upper extremities. The initial trauma radiographic series demonstrated, on the anteroposterior chest projection, an asymmetric bilateral glenohumeral dislocation (Fig. 1).
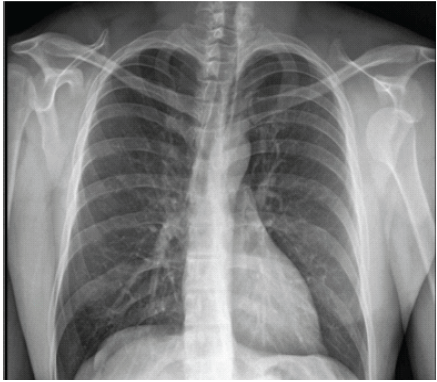
Figure 1: Anteroposterior chest radiograph showing asymmetric bilateral shoulder dislocation.
Targeted shoulder radiographs revealed an anterior subglenoid dislocation of the left shoulder (Fig. 2) and a posterior dislocation of the right shoulder (Fig. 3).
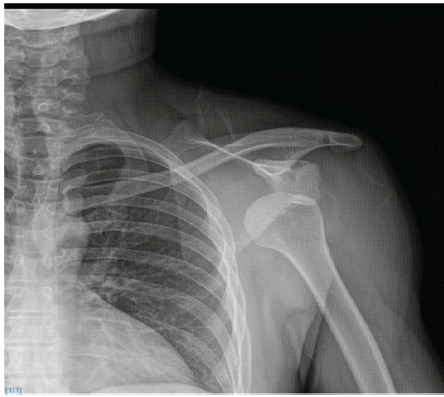
Figure 2: Anteroposterior radiograph of the left shoulder demonstrating anterior subglenoid dislocation.
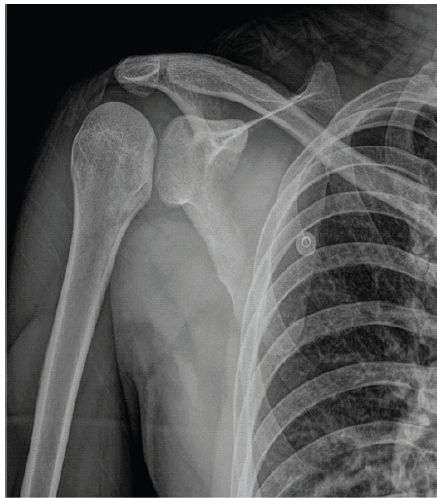
Figure 3: Anteroposterior radiograph of the right shoulder showing posterior dislocation with the light bulb sign and presence of the glenoid rim sign (vacant glenoid).
Computed tomography confirmed a non-engaging reverse Hill–Sachs lesion involving approximately 18% of the articular surface of the right humeral head (Fig. 4).
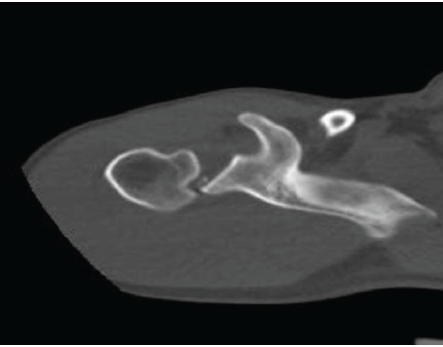
Figure 4: Axial computed tomography scan of the right shoulder showing a reverse Hill–Sachs lesion associated with posterior dislocation.
Under conscious sedation with diazepam and midazolam, bilateral closed reduction was performed using the Kocher manoeuvre for the left shoulder and the Wilson manoeuvre for the right shoulder, achieving adequate joint congruency (Fig. 5).
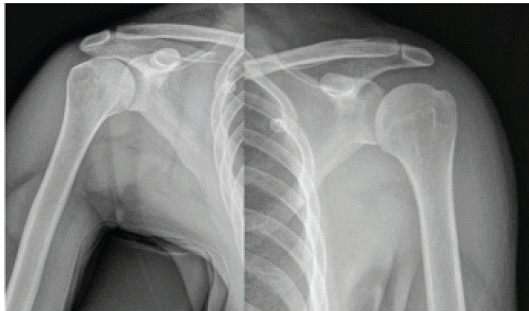
Figure 5: Post-reduction anteroposterior radiographs of both shoulders.
Subsequently, a universal shoulder immobiliser was applied to the left shoulder and an abduction pillow to the right shoulder, along with analgesic management using non-steroidal anti-inflammatory drugs. The patient was discharged with outpatient follow-up. Immobilisation of the left shoulder was discontinued after 2 weeks and the abduction pillow of the right shoulder after 3 weeks. A physical rehabilitation programme was then initiated, including pendulum exercises, progressive isometric strengthening, thermotherapy, and therapeutic ultrasound. During follow-up, progressive improvement in pain and range of motion was observed. At 3 months, shoulder flexion and abduction reached 160° in the right shoulder and 140° of flexion with 145° of abduction in the left shoulder, with preserved muscle strength and trophism. Functional assessment using the DASH questionnaire showed scores of 15 points for the right shoulder and 20 points for the left shoulder, improving to 8 and 9 points, respectively, at 6 months. This improvement was associated with complete recovery of the range of motion (Fig. 6) and absence of complications.
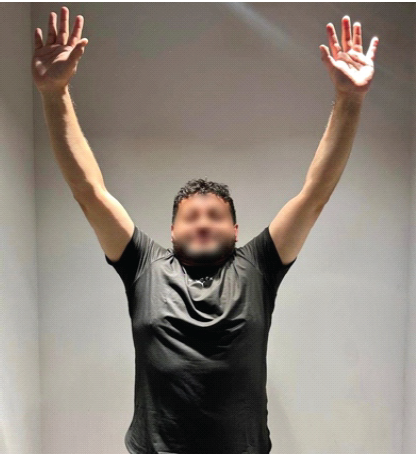
Figure 6: Final active range of motion of both shoulders at 6 months of follow-up.
Asymmetric bilateral shoulder dislocations are extremely rare injuries. The most commonly reported presentation involves opposite directions (anterior–posterior). The main mechanism of injury described in the literature is seizure activity, whereas other etiological mechanisms, such as electrical shock, have been reported only exceptionally, with a single documented case. The traumatic mechanisms described in the literature predominantly involve low-energy events or combined mechanisms. To our knowledge, the present case represents the first report of asymmetric bilateral shoulder dislocation secondary to a pure high-energy traumatic mechanism [4,5,6,7,8,9,10,11,12]. These injuries are frequently associated with fractures of the proximal humerus, glenoid rim injuries, or rotator cuff lesions, which increase both diagnostic and therapeutic complexity as well as the risk of long-term functional sequelae [4,5,6,8,9,10,12]. In contrast, no associated fractures were identified in the present case, which allowed for conservative management following stable closed reduction, with satisfactory functional outcomes. These findings are consistent with those reported by Özer et al. and Lehreitani et al. in selected cases successfully treated without surgical intervention [5,9]. From a diagnostic perspective, isolated anteroposterior radiographs are often insufficient to identify posterior shoulder dislocation, particularly in bilateral presentations or in polytrauma patients, which may lead to delayed diagnosis [14,15]. For this reason, the initial evaluation should be complemented with scapular “Y” and axillary views, which significantly increase diagnostic sensitivity. In selected cases, computed tomography plays a crucial role in accurately defining the dislocation pattern and detecting associated osseous injuries, such as Hill–Sachs or reverse Hill–Sachs lesions, thereby optimising therapeutic planning [15,16]. Post-reduction management of asymmetric bilateral shoulder dislocations is not standardised due to the rarity of this condition. In the absence of specific guidelines, treatment is generally based on the established principles for anterior, posterior, and inferior glenohumeral dislocations, which are considered as independent entities. These principles guide decisions regarding the type and duration of immobilisation as well as the gradual initiation of functional rehabilitation [16,17,18]. Regarding reduction techniques, the literature suggests that the most appropriate manoeuvre is the one with which the clinician is most familiar, provided that biomechanical and safety principles are respected, particularly in complex bilateral scenarios [14,15,16]. In the present case, the use of a universal shoulder immobiliser for the anteriorly dislocated shoulder and an abduction pillow for the posteriorly dislocated shoulder provided adequate protection during the acute phase. Subsequently, the initiation of a supervised rehabilitation programme facilitated progressive recovery of range of motion and muscle strength, without evidence of residual instability or complications, with outcomes comparable to those previously reported in the literature [4,7]. An important aspect of this report is the objective functional assessment using the DASH questionnaire. Unlike most previously reported cases, in which outcomes were described subjectively, only Diniz et al. used the Constant–Murley score to evaluate functional recovery [12]. Finally, DASH scores lower than 10 points are considered compatible with normal or near-normal upper-limb function [19,20], which is consistent with the results obtained in this case.
Asymmetric bilateral shoulder dislocation is an exceptionally rare entity whose diagnosis and management represent a significant clinical challenge. The present case constitutes the first documented report in Mexico of asymmetric bilateral shoulder dislocation secondary to a high-energy traumatic mechanism without associated osseous injuries, thereby expanding the previously described etiological spectrum. This case highlights the importance of maintaining a high index of diagnostic suspicion, particularly in complex traumatic scenarios, as well as the need to complement the initial radiographic evaluation with specific projections and computed tomography to avoid missed diagnoses, especially of posterior shoulder dislocation. In the absence of associated fractures or persistent instability, individualised conservative management based on the accepted principles for each type of glenohumeral dislocation can provide satisfactory functional outcomes. The use of a validated functional scale, such as the DASH questionnaire, adds further value by allowing an objective and reproducible assessment of recovery, an aspect that remains scarcely documented in the existing literature.
Asymmetric bilateral shoulder dislocation is an extremely rare injury that can be overlooked in high-energy trauma. Careful clinical assessment and appropriate radiographic evaluation, including axillary or scapular Y views, are essential for early diagnosis and appropriate management.
References
- 1. Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am 2010;92:542-9. [Google Scholar] [PubMed]
- 2. Robinson CM, Aderinto J. Recurrent posterior shoulder instability. J Bone Joint Surg Am 2005;87:883-92. [Google Scholar] [PubMed]
- 3. Aufderheide TP, Frascone RJ, Cicero JJ. Simultaneous bilateral anterior and posterior shoulder dislocations. Am J Emerg Med 1985;3:331-3. [Google Scholar] [PubMed]
- 4. Tsionos I, Karahalios T, Zibis AH, Malizos KN. Combined anterior and posterior shoulder dislocation as a manifestation of a brain tumour. Acta Orthop Belg 2004;70:612-5. [Google Scholar] [PubMed]
- 5. Özer H, Baltaci G, Selek H, Turanli S. Opposite-direction bilateral fracture dislocation of the shoulders after an electric shock. Arch Orthop Trauma Surg 2005;125:499-502. [Google Scholar] [PubMed]
- 6. Fung DA, Menkowitz M, Chern K. Asymmetric bilateral shoulder dislocation involving a luxatio erecta dislocation. Am J Orthop 2008;37:E97-8. [Google Scholar] [PubMed]
- 7. Nema SK, Pai DR, Sinha NK, Gupta KK. A unique case of non-traumatic asymmetric shoulder dislocation with four-part fractures of proximal humeri following seizures. J Emerg Trauma Shock 2013;6:231-2. [Google Scholar] [PubMed]
- 8. Sharma D, Karthikeyan M, Natraj AR, Poduval M, Patro DK. Asymmetrical fracture dislocation of shoulder – a case report and review of literature. J Orthop Case Rep 2013;3:19-22. [Google Scholar] [PubMed]
- 9. Lehreitani ML, Abid H, Marcaillou F, Sidat B, El Ibrahimi A, Elmrini A, et al. A new case of opposite-direction bilateral shoulder fracture-dislocation (case study and review). Sch J Med Case Rep 2017;5:422-6. [Google Scholar] [PubMed]
- 10. Sharma A, Jindal S, Narula MS, Garg S, Sethi A. Bilateral asymmetrical fracture dislocation of shoulder with rare combination of injuries after epileptic seizure: A case report. Malays Orthop J 2017;11:74-6. [Google Scholar] [PubMed]
- 11. Alsuwayh WM, Ahmed HAE. Bilateral anterior and posterior shoulder dislocation: Case report. Egypt J Hosp Med 2022;89:4308-11. [Google Scholar] [PubMed]
- 12. Diniz SE, Vale J, Fonte H, Xará-Leite F, Barros LH, Claro R. Asymmetric bilateral chronic shoulder dislocation in a young patient: A rare case report. J Orthop Case Rep 2022;12:91-6. [Google Scholar] [PubMed]
- 13. Kang T, Shin WJ, Lee SG. Bilateral asymmetric fracture dislocation of shoulder after hypoglycemic shock. J Korean Orthop Assoc 2023;58:67-72. [Google Scholar] [PubMed]
- 14. Cicak N. Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-32. [Google Scholar] [PubMed]
- 15. Hawkins RJ, Neer CS 2nd, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. [Google Scholar] [PubMed]
- 16. Rockwood CA Jr., Matsen FA 3rd, Wirth MA, Lippitt SB. The Shoulder. 4th ed. Philadelphia, PA: Saunders Elsevier; 2009. [Google Scholar] [PubMed]
- 17. Itoi E, Hatakeyama Y, Kido T, Sato T, Minagawa H, Yamamoto N. Immobilization in external rotation after shoulder dislocation. J Bone Joint Surg Am 2003;85:418-25. [Google Scholar] [PubMed]
- 18. Mallon WJ, Bassett FH 3rd, Goldner RD. Luxatio erecta: The inferior glenohumeral dislocation. J Orthop Trauma 1990;4:19-24. [Google Scholar] [PubMed]
- 19. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The upper extremity collaborative group (UECG). Am J Ind Med 1996;29:602-8. [Google Scholar] [PubMed]
- 20. Gummesson C, Atroshi I, Ekdahl C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet Disord 2003;4:11. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Simultaneous Bilateral Anterior Shoulder Dislocation Following Epileptic Seizure in a Middle-Aged Male: A Rare Case Report and Review of Literature
October 1, 2025 Simultaneous Bilateral Anterior Shoulder Dislocation Following Epileptic Seizure in a Middle-Aged Male: A Rare Case Report and Review of Literature September 1, 2025 Irreducible Anterior Shoulder Dislocation with Greater Tuberosity Fracture: Joystick Reduction and Biceps Preservation in an Elderly Female -A Case Report
September 1, 2025 Irreducible Anterior Shoulder Dislocation with Greater Tuberosity Fracture: Joystick Reduction and Biceps Preservation in an Elderly Female -A Case Report August 1, 2025 Complex Scapulothoracic Disruption Managed with Scapular Dual Column Plating and Acromion Tension Band Osteosynthesis: A Radiological and Functional Success Story
August 1, 2025 Complex Scapulothoracic Disruption Managed with Scapular Dual Column Plating and Acromion Tension Band Osteosynthesis: A Radiological and Functional Success Story March 1, 2025 Anterior Hip Dislocation Following Total Hip Arthroplasty, Caused by Broken Trial Femoral Head Particles: A Case Report
March 1, 2025 Anterior Hip Dislocation Following Total Hip Arthroplasty, Caused by Broken Trial Femoral Head Particles: A Case Report