
Chronic non-infective osteomyelitis should be considered in immunocompromised patients presenting with bilateral multifocal cystic foot swellings, osteomyelitis-like MRI features, and persistently sterile microbiological studies.
Dr Harish Kiran, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: harishkiran.2694@gmail.com
Abstract
Introduction: We report an unusual case of bilateral multiloculated cystic foot swellings in which extensive investigations failed to establish a definitive diagnosis, highlighting the challenges in distinguishing culture-negative infectious osteomyelitis from chronic non-infective osteomyelitis. Chronic osteomyelitis typically presents with a localised infection and an identifiable microbiological aetiology. However, atypical presentations with bilateral involvement and sterile cultures pose significant diagnostic challenges, especially in immunocompromised individuals.
Case Report: A 56-year-old female presented with multiple bilateral foot swellings of 2 years' duration, associated with pain. Clinical examination revealed well-defined cystic, fluctuant swellings without classical signs of infection. Magnetic resonance imaging (MRI) demonstrated multiloculated fluid collections with sinus tracts and adjacent bony involvement suggestive of chronic osteomyelitis. Despite aspiration and biopsy, microbiological studies remained negative. Histopathology revealed acute-on-chronic inflammatory granulation tissue. The patient had significant comorbidities, including diabetes mellitus, rheumatoid arthritis, and prolonged steroid use.
Conclusion: Although MRI findings were highly suggestive of chronic osteomyelitis, persistently negative microbiological studies and non-specific histopathology precluded definitive confirmation of infection. After extensive multidisciplinary evaluation, chronic non-infective osteomyelitis emerged as the most plausible diagnosis. This case represents a significant diagnostic dilemma.
Keywords: Chronic osteomyelitis, culture-negative, bilateral foot swelling, magnetic resonance imaging, steroid misuse, diagnostic dilemma.
Chronic osteomyelitis is a persistent infection of bone characterised by necrosis, sequestrum formation, and chronic inflammatory changes. It is most commonly caused by bacterial pathogens; however, a subset of patients present with culture-negative osteomyelitis, complicating diagnosis and management [1,2]. Bilateral involvement of the foot is uncommon and may mimic benign cystic lesions, inflammatory arthropathies, or neoplastic conditions [3]. Furthermore, immunocompromised states such as diabetes, autoimmune diseases, and prolonged corticosteroid use can alter disease presentation and obscure classical clinical features [4]. We report a rare case of bilateral multiloculated cystic foot swellings with radiological features suggestive of osteomyelitis but persistently negative microbiological findings, highlighting the diagnostic dilemma and the importance of clinicoradiological correlation.
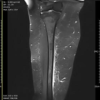
A 56-year-old female presented with complaints of multiple swellings over both feet for 2 years, associated with pain for the past 1 year. Swelling initially appeared in the left foot and gradually progressed to involve both feet with multiple swellings over a period of 4 years. The pain was insidious in onset, pricking and burning in nature, gradually progressive, aggravated by walking and standing, and relieved with medications. There was no associated history of fever, discharge, sinus formation, trauma, or thorn prick. No history of barefoot walking. She had a history of prolonged unsupervised steroid intake for pain relief. She was a known case of diabetes mellitus, systemic hypertension, and rheumatoid arthritis. On clinical examination, she had multiple globular swellings that were present over the dorsoplantar junction of both feet. The swellings were well-defined, cystic, fluctuant, and non-mobile. There was no local warmth, erythema, or discharge. Mild tenderness was noted. Ankle range of motion was full and painless. Toe movements were preserved. No distal neurovascular deficit was present. Laboratory findings were a normal total leukocyte count (8860) with elevated erythrocyte sedimentation rate (88 mm/h) and C-reactive protein (2.4 mg/L). Radiology showed no significant bony abnormality but showed multiple soft-tissue shadows along the plane of swelling. Magnetic resonance imaging (MRI) of the right foot revealed multiloculated thick-walled fluid collections in the plantar aspect of the hindfoot with multiple branching sinus tracts extending along subcutaneous and intermuscular planes. A cortical breach with marrow oedema was noted in the cuboid, with extension to adjacent bones, including the base of the fifth metatarsal and calcaneum. Extensive surrounding soft-tissue oedema was present. These findings were suggestive of a chronic infective aetiology with osteomyelitis.
Procedures:
Initially, aspiration of a single swelling over the right foot was done, from which approximately 20 mL of straw-coloured fluid was aspirated. Culture showed no growth. Notably, swelling reaccumulated within 24 h after aspiration. Later, we did an open biopsy of swelling over the right foot, which revealed occasional pus cells without identifiable organisms in gram stain and was negative for bacterial culture, fungal culture, acid-fast bacilli, GeneXpert, and potassium hydroxide (KOH) mount. Histopathology revealed acute-on-chronic inflammatory granulation tissue composed of neutrophils, lymphocytes, vascular proliferation, and pigment-laden macrophages, suggestive of chronic inflammatory pathology. Detailed evaluation by rheumatology and dermatology specialists did not reveal evidence of active systemic inflammatory disease, extra-articular rheumatoid manifestations, or cutaneous lesions suggestive of alternative diagnoses. The patient was treated with empirical broad-spectrum antibiotics and followed for six months. During follow-up, she reported a gradual reduction in pain and swelling, with no development of new lesions.
Chronic osteomyelitis is traditionally regarded as an infective condition; however, its presentation can vary widely, particularly in immunocompromised individuals [5]. The present case is notable for its bilateral involvement, cystic morphology, and persistently negative microbiological findings, all of which contribute to a significant diagnostic dilemma. An important consideration in such cases is chronic non-infective osteomyelitis, a sterile inflammatory disorder characterised by immune-mediated bone inflammation.¹ Although more commonly described in paediatric populations, adult presentations – particularly in association with autoimmune diseases such as rheumatoid arthritis – are increasingly recognised [2]. The bilateral and multifocal nature of the lesions in this patient, along with negative cultures, raises the possibility of a non-infective inflammatory process. However, several features in this case strongly favour an infective aetiology. MRI demonstrated multiloculated collections, sinus tract formation, cortical breach, and marrow oedema, which are characteristic of chronic osteomyelitis [3,6]. Imaging plays a pivotal role in such scenarios, as MRI has high sensitivity for detecting early bone and soft-tissue involvement, although its specificity remains limited [7]. Therefore, radiological findings must be interpreted in conjunction with clinical and histopathological data. The persistently culture-negative status observed in this patient is not uncommon, with literature reporting rates of up to 30% [2,8]. This may be attributed to prior antibiotic exposure, low-virulence organisms, or inadequate sampling. In addition, prolonged corticosteroid use in this patient likely contributed to immune suppression, masking classical signs of infection and potentially leading to sterile cultures [4]. Another rare but relevant differential diagnosis is pseudohyphomycotic cyst [9], a form of subcutaneous fungal infection seen in immunocompromised hosts. These lesions may present as chronic, cystic swellings mimicking benign or infective conditions. However, the absence of fungal elements on histopathology, along with negative KOH and culture studies, makes this diagnosis unlikely in the present case. Ganglion cysts [10] may present as cystic, occasionally multiloculated lesions; however, the presence of sinus tracts, marrow oedema, and cortical breach in this case is atypical. A synovial cyst was also considered, but the absence of a clear communication with the adjacent joint or tendon sheath on imaging made this diagnosis unlikely. In addition, the lesions lacked synovial lining on histopathology, arguing against a synovial cyst. Mycetoma was ruled out, as there were absent discharging sinuses, granules, and a typical “dot-in-circle” [11] sign on MRI, which argued against this diagnosis. Furthermore, no fungal elements or grains were identified on cytology/biopsy, making mycetoma unlikely. Rheumatoid nodules were considered, given the background of rheumatoid arthritis; however, the atypical bilateral plantar distribution and imaging characteristics were not classical. Moreover, histopathology did not demonstrate well-formed palisading granulomas [12] with central fibrinoid necrosis, making this diagnosis less likely. It went against the favour of Ledderhose disease [13], as the lesions were not confined to the plantar fascia and lacked the typical cord-like fibromatosis pattern on imaging. In addition, histopathology did not show dense fibroblastic proliferation with collagen deposition, making this diagnosis unlikely. Neoplasm was ruled out from considerations, as neither imaging showed a discrete aggressive mass, bone destruction, or invasive features, nor did histopathology reveal cellular atypia, pleomorphism, or mitotic activity, effectively ruling out a neoplastic aetiology. The presence of bone involvement and sinus tract formation effectively excludes most benign cystic conditions and favours an underlying infective process. Thus, this case represents a complex diagnostic dilemma. Although infectious osteomyelitis remained a strong consideration based on MRI findings, persistently negative microbiological studies and non-specific histopathology prevented definitive confirmation. Chronic non-infective osteomyelitis appears to be the most plausible diagnosis after exclusion of other differentials with atypical cystic presentation, occurring in an immunocompromised host. It underscores the importance of maintaining a high index of suspicion and relying on a combination of clinical, radiological, and histopathological findings for diagnosis. Bilateral multiloculated cystic swellings of the foot with negative microbiological studies represent a significant diagnostic challenge. Chronic non-infective osteomyelitis should be strongly considered in such cases, particularly in immunocompromised patients. MRI and histopathology play a crucial role in establishing the diagnosis when cultures are inconclusive.
Limitations:
This report describes a single unusual case and is intended to highlight a diagnostic challenge rather than provide generalisable conclusions. Definitive microbiological confirmation was not obtained despite extensive testing and advanced molecular diagnostics. Additional imaging modalities such as positron emission tomography-computed tomography or bone scintigraphy was not performed due to financial constraints. Although only one representative lesion underwent open biopsy, the bilateral lesions were clinically and radiologically similar. The patient was followed for six months, during which symptoms improved with empirical antibiotic therapy; however, the final diagnosis remains presumptive.
Bilateral multifocal cystic foot swellings with osteomyelitis-like imaging findings represent a rare and challenging diagnostic entity. Differential diagnoses include infective chronic osteomyelitis, chronic non-infective osteomyelitis (CNO), mycetoma, ganglion cyst, synovial cyst, rheumatoid nodules, pseudohyphomycosis, Ledderhose disease, inflammatory arthropathies, and soft-tissue neoplasms. In the present case, chronic non-infective osteomyelitis emerged as the most plausible diagnosis owing to bilateral multifocal involvement, persistently sterile microbiological studies, non-specific histopathology, absence of definitive infective or neoplastic pathology, and clinicoradiological features suggestive of a sterile inflammatory process. This case highlights the importance of integrating clinical, radiological, microbiological, and histopathological findings while evaluating atypical bilateral foot lesions in immunocompromised patients.
In patients presenting with bilateral cystic foot swellings and sterile microbiological studies, chronic non-infective osteomyelitis should be considered alongside infectious osteomyelitis. Diagnosis requires careful clinicoradiological and histopathological correlation, particularly in immunocompromised individuals.
References
- 1. Lew DP, Waldvogel FA. Osteomyelitis. Lancet 2004;364:369-79. [Google Scholar] [PubMed]
- 2. Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am 2005;19:765-86. [Google Scholar] [PubMed]
- 3. Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: The role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin Plast Surg 2009;23:80-9. [Google Scholar] [PubMed]
- 4. Kaplan SL. Bone and joint infections. J Infect 2014;68:S51-6. [Google Scholar] [PubMed]
- 5. Zimmerli W. Clinical practice. Vertebral osteomyelitis. N Engl J Med 2010;362:1022- [Google Scholar] [PubMed]
- 6. Termaat MF, Raijmakers PG, Scholten HJ, Bakker FC, Patka P, Haarman HJ. The accuracy of diagnostic imaging for the assessment of chronic osteomyelitis: A systematic review and meta-analysis. J Bone Joint Surg Am 2005;87:2464-71. [Google Scholar] [PubMed]
- 7. Palestro CJ, Love C, Miller TT. Imaging of musculoskeletal infections. Best Pract Res Clin Rheumatol. 2006;20:1197-1218 [Google Scholar] [PubMed]
- 8. Senneville E, Robineau O, Valette M, Beltrand E, Legout L, Caillaux M. Culture-negative osteomyelitis. Int J Infect Dis. 2012;16:e406-11. [Google Scholar] [PubMed]
- 9. McGinnis MR. Phaeohyphomycosis and hyalohyphomycosis. Mycopathologia. 1983;81:3-19. [Google Scholar] [PubMed]
- 10. Neto N, Nunnes P. Spectrum of MRI features of ganglion and synovial cysts. Insights Imaging 2016;7:179-86. [Google Scholar] [PubMed]
- 11. Sarris I, Berendt AR, Athanasous N, Ostlere SJ. The MRI ‘dot-in-circle’ sign in mycetoma: A characteristic finding. AJR Am J Roentgenol. 2003;180:357-59. [Google Scholar] [PubMed]
- 12. Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 10th ed. Netherlands: Elsevier; 2020. [Google Scholar] [PubMed]
- 13. De Palma L, Angelini A, Pavan M, Zanus G. Plantar fibromatosis (Ledderhose disease): MR imaging findings. Radiol Med. 1999;98:117-20. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma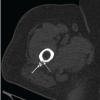 August 1, 2026 Calcific Tendinitis of the Linea Aspera with Bilateral Deposits and Inflammatory Asymmetry Presenting as Unilateral Pain: A Case Report and Review of Literature
August 1, 2026 Calcific Tendinitis of the Linea Aspera with Bilateral Deposits and Inflammatory Asymmetry Presenting as Unilateral Pain: A Case Report and Review of Literature August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report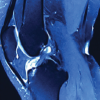 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain