
Discordant imaging and biopsy findings in cartilaginous bone tumours should prompt repeat biopsy and multidisciplinary evaluation, as accurate clinico-radiological correlation is essential to distinguish enchondroma from low-grade chondrosarcoma and guide appropriate treatment.
Dr. S Depak Charan, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: depakcharan@yahoo.in
Abstract
Introduction: Differentiating enchondroma from low-grade chondrosarcoma remains challenging due to significant overlap in clinical presentation, imaging characteristics, and histopathological appearance. Accurate diagnosis is crucial in guiding appropriate treatment and preventing unnecessary aggressive management.
Case Report: A 25-year-old female presented with progressive right knee pain for 20 days. The X-ray was inconclusive. Magnetic resonance imaging demonstrated a well-defined intramedullary lesion within the distal femur measuring approximately 7.6 × 2.6 × 3 cm. Initial computed tomography (CT)-guided biopsy results were inconclusive. Repeat imaging, including magnetic resonance imaging and positron emission tomography-CT, suggested a non-aggressive lesion without metastatic disease. After multidisciplinary tumour board discussion, a repeat biopsy demonstrated a cartilaginous neoplasm compatible with enchondroma. The patient subsequently underwent intralesional curettage with antibiotic-loaded bone cement filling. Final histopathological analysis confirmed a benign enchondroma.
Conclusion: This report highlights the importance of clinicoradiological correlation and repeat biopsy when initial investigations provide conflicting information in suspected cartilage tumours.
Keywords: Enchondroma, distal femur tumour, intramedullary cartilage tumour, low-grade chondrosarcoma, bone tumour biopsy, diagnostic dilemma, curettage and cementation, musculoskeletal oncology.
Cartilaginous tumours of bone represent a spectrum of lesions ranging from benign enchondromas to malignant chondrosarcomas. Accurate differentiation between these entities remains a well-known challenge in orthopaedic oncology because they share overlapping clinical, radiological, and histopathological characteristics [1,2,3]. Although enchondromas are benign lesions, low-grade chondrosarcomas may present with similar imaging findings. Enchondromas are intramedullary tumours composed of hyaline cartilage arising from residual cartilage rests in the bone marrow cavity. These lesions most frequently occur in the metaphyseal or diaphyseal regions of long bones and are often discovered incidentally during imaging studies performed for unrelated conditions [1]. While many enchondromas remain asymptomatic, some patients may present with pain, swelling, or a pathological fracture. The presence of persistent pain in a cartilage tumour located in a weight-bearing bone, such as the femur, raises concern for malignancy. Low-grade chondrosarcoma represents a slow-growing malignant cartilage tumour that may closely resemble an enchondroma on both radiological and histological examination [2]. Radiological signs suggesting malignancy include endosteal scalloping involving more than two-thirds of cortical thickness, cortical disruption, periosteal reaction, and soft-tissue extension [4,5]. Histopathological diagnosis can also be challenging because cartilage tumours frequently demonstrate variable cellularity and architecture. Sampling errors or inadequate biopsy specimens may lead to inconclusive or misleading results. Consequently, management decisions should rely on a combination of clinical presentation, imaging findings, histopathology, and multidisciplinary discussion. This report describes a case of distal femoral enchondroma presenting as a diagnostic dilemma due to discordant biopsy findings, emphasising the role of repeat biopsy and comprehensive evaluation in establishing the correct diagnosis.
A 25-year-old female presented to the orthopaedic outpatient department complaining of pain in the right knee for approximately 20 days. The pain had developed gradually without any identifiable precipitating event. It was described as a dull aching discomfort localised around the knee joint without radiation. The symptoms progressively increased over time and were not associated with any specific aggravating or relieving factors. There was no history of trauma, fever, weight loss, night pain, or systemic symptoms. The patient denied any previous similar complaints or underlying medical conditions. Her past medical and family history was unremarkable.
Clinical examination:
Physical examination revealed no visible deformity or swelling around the knee. There were no scars, sinus tracts, or dilated superficial veins. Palpation demonstrated localised tenderness over the anterior aspect of the distal femur. No local warmth was detected. The range of motion of the knee joint was from full extension to approximately 100° of flexion, with mild discomfort during deeper flexion. Sensory examination of the limb was normal, and distal pulses were palpable. Based on the clinical findings, a benign bone lesion such as fibrous dysplasia was initially suspected.
Initial imaging and biopsy:
The initial X-ray taken was found to be inconclusive (Figure 1).

Figure 1: Initial plain radiograph of the right knee joint (anteroposterior and lateral views) showing no definite abnormality in the distal femur. The lesion was not clearly appreciable on radiographs.
Magnetic resonance imaging of the right knee performed at an outside facility demonstrated a well-circumscribed, lobulated intramedullary lesion located in the distal femoral metaphyseal-diaphyseal region. The lesion measured approximately 7.6 cm in craniocaudal length, 2.6 cm transversely, and 3 cm in the anteroposterior dimension. On magnetic resonance imaging (MRI) sequences, the lesion appeared hypointense on T1-weighted images and hyperintense on short tau inversion recovery sequences. No cortical destruction, periosteal reaction, or surrounding soft-tissue mass was identified. The radiological differential diagnosis included enchondroma, low-grade chondrosarcoma, and simple bone cyst [6]. A computed tomography (CT)-guided biopsy was performed right after MRI. Histopathological analysis revealed necrotic osteoid tissue without identifiable tumour cells. As the findings were inconsistent with imaging characteristics, the biopsy slides were reviewed at another laboratory for a second opinion. The second report described fibrous tissue with areas of calcification and hyalinisation, along with scattered normal bony trabeculae. No malignant cells or granulomatous inflammation was identified. These findings remained inconclusive.
Further evaluation:
The patient subsequently presented to our institution after 1 week for further management. Repeat MRI performed demonstrated a well-defined non-aggressive intramedullary lesion involving the middle and distal femoral diaphysis (Figure 2).
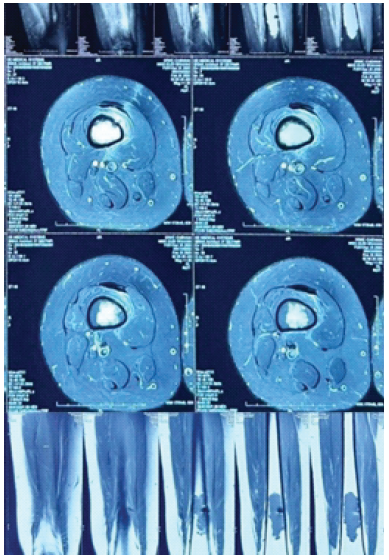
Figure 2 Repeat magnetic resonance imaging of the right femur with knee screening performed at our institution, demonstrating a well-defined lobulated intramedullary lesion involving the mid and distal femoral diaphysis. The lesion appears hypointense on T1-weighted sequences and hyperintense on T2/short tau inversion recovery images without significant cortical destruction, periosteal reaction, or soft-tissue extension, features suggestive of a benign cartilaginous lesion, likely an enchondroma.
The imaging characteristics were consistent with a benign cartilage tumour, most likely an enchondroma. To further evaluate metabolic activity, a positron emission tomography-CT (PET-CT) scan was obtained the next day (Figure 3).
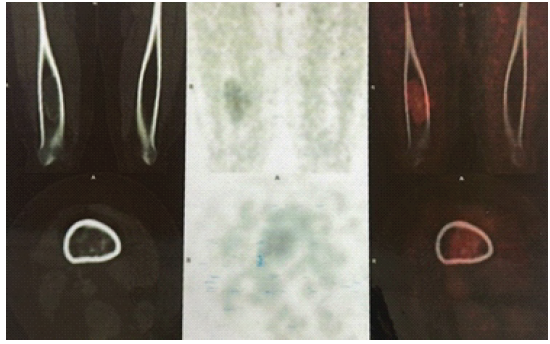
Figure 3 18F-fluorodeoxyglucose positron emission tomography-computed tomography scan demonstrating focal low-grade metabolic uptake within the intramedullary lesion of the distal right femur (standardized uptake value max ~2.6). No additional metabolically active lesions or distant metastases are identified elsewhere in the body, supporting the likelihood of a benign cartilaginous lesion.
The study demonstrated low-grade fluorodeoxyglucose uptake with a maximum standardised uptake value (SUV) of approximately 2.6 within the lesion. No additional metabolically active lesions or distant metastases were detected. Low metabolic activity on PET-CT has been associated with benign cartilage tumours, further supporting the diagnosis of enchondroma [7]. Given the discrepancy between imaging findings and biopsy results, the case was discussed in a multidisciplinary tumour board meeting, including orthopaedic oncologists, radiologists, medical oncologists, and radiation oncologists. Considering the persistent symptoms, inconclusive histopathology, and imaging findings suggestive of a benign lesion, the tumour board recommended performing a repeat CT-guided biopsy to obtain a more representative tissue sample. Repeat CT-guided biopsy was planned and performed after 1 week. Histological examination demonstrated cartilage fragments composed of chondrocytes embedded within a hyaline matrix without features of malignancy. These findings were consistent with a cartilaginous neoplasm suggestive of enchondroma. Based on the biopsy findings and tumour board recommendation, surgical treatment was planned. After 5 days with all the required fitness for surgery, the patient underwent tumour excision with intralesional curettage of the distal femoral lesion (Figure 4).
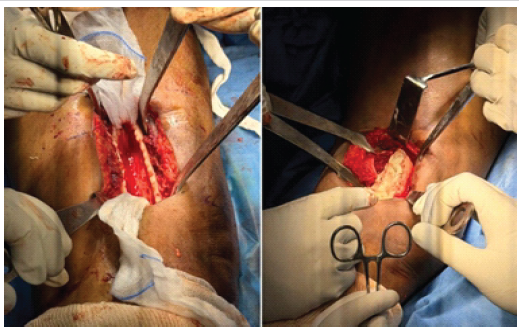
Figure 4 Intraoperative clinical photographs demonstrating exposure of the distal femur lesion through a cortical window with intralesional curettage of the tumor cavity, followed by filling of the defect with antibiotic-loaded polymethylmethacrylate bone cement.
The resulting cavity was filled with antibiotic-loaded polymethylmethacrylate bone cement. Intralesional curettage combined with bone cement filling is widely used in the management of symptomatic enchondromas. Cement provides immediate mechanical stability, facilitates early mobilisation, and allows easier radiographic detection of recurrence during follow-up (Figure 5) [8,9,10,11].

Figure 5 Post-operative plain radiograph of the right femur (anteroposterior and lateral views) demonstrating the distal femoral cavity following intralesional curettage, filled with antibiotic-loaded polymethylmethacrylate bone cement. The cement occupies the tumor cavity with maintained cortical integrity and satisfactory post-operative alignment.
The excised tissue specimen was sent for definitive histopathological examination (Figure 6).
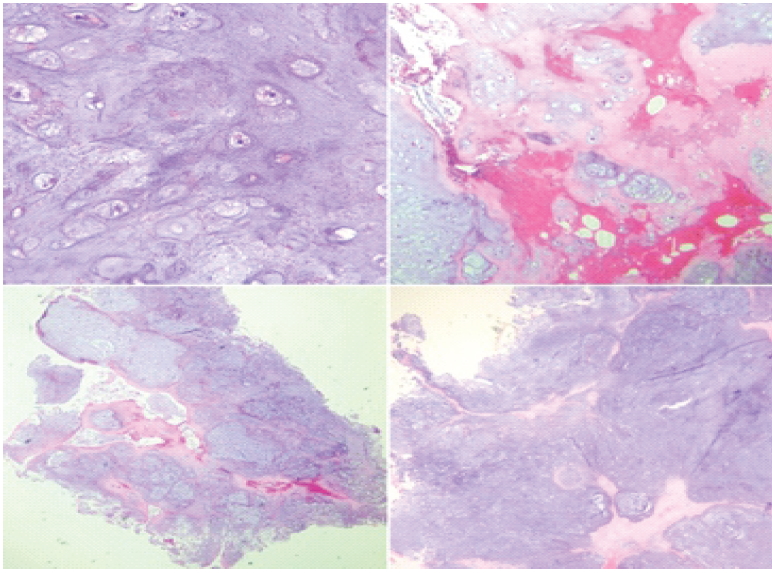
Figure 6 Histopathological photomicrographs (hematoxylin and eosin staining) demonstrating lobules of mature hyaline cartilage separated by fibrous septae. The chondrocytes are seen within well-formed lacunae exhibiting bland cytological features with relatively small, uniform nuclei and inconspicuous nucleoli. Occasional binucleated chondrocytes are present without significant nuclear atypia, increased mitotic activity, or necrosis. These findings are consistent with a benign cartilaginous lesion suggestive of enchondroma.
Microscopic evaluation revealed lobules of mature hyaline cartilage containing chondrocytes located within lacunae. The cells exhibited bland nuclear morphology without atypia, mitotic activity, or necrosis. These findings confirmed the diagnosis of a benign cartilaginous tumour consistent with enchondroma.
Distinguishing enchondroma from low-grade chondrosarcoma remains a difficult diagnostic problem in musculoskeletal oncology [12]. Both lesions share similar clinical manifestations and imaging appearances, which often complicates clinical decision-making. Pain has historically been considered a feature suggestive of malignancy in cartilage tumours. However, several studies have reported that benign enchondromas may also produce pain due to mechanical stress, cortical thinning, or associated bone marrow oedema [2]. Therefore, clinical symptoms alone cannot reliably distinguish between benign and malignant lesions. Radiological evaluation remains an essential component of the diagnostic process. Enchondromas typically appear as well-defined intramedullary lesions with chondroid matrix calcifications and minimal cortical involvement. In contrast, low-grade chondrosarcomas may demonstrate cortical destruction, extensive endosteal scalloping, periosteal reaction, and soft-tissue extension [4,5]. In the present case, MRI consistently demonstrated a well-defined intramedullary lesion without aggressive radiological features. These findings strongly favoured a benign cartilage tumour. Histopathological examination is traditionally considered the gold standard for diagnosis. Nevertheless, biopsy interpretation may be complicated by sampling error, tumour heterogeneity, or insufficient tissue. Small biopsy specimens may not adequately represent the entire lesion, potentially resulting in inconclusive findings. This challenge was illustrated in our case, where the initial biopsy failed to demonstrate tumour tissue. Only after a repeat biopsy was the cartilaginous nature of the lesion identified. PET-CT has recently been explored as an adjunct tool for differentiating benign from malignant cartilage tumours. Previous studies have suggested that lesions demonstrating low SUVs are more likely to represent benign pathology [7]. In our patient, the SUV value of approximately 2.6 further supported a benign diagnosis. The standard treatment for symptomatic enchondromas involves intralesional curettage followed by bone grafting or cementation. Bone cement provides immediate structural support and allows early weight-bearing. In addition, recurrence can be easily detected due to the contrast between cement and surrounding bone on radiographs. This case emphasises the importance of integrating clinical evaluation, imaging findings, histopathological analysis, and multidisciplinary discussion in the management of cartilage tumours [8,9,10,11,13].
Cartilage tumours of long bones may present significant diagnostic challenges due to overlapping features between benign enchondromas and low-grade chondrosarcomas. When imaging findings and biopsy results are inconsistent, repeat biopsy and multidisciplinary evaluation are essential to establish an accurate diagnosis. Appropriate clinicoradiological correlation helps guide optimal treatment and prevents unnecessary aggressive interventions.
Discordant imaging and biopsy findings in suspected cartilage tumours should prompt repeat biopsy and multidisciplinary evaluation to avoid misdiagnosis and inappropriate treatment.
References
- 1. Walden MJ, Murphey MD, Vidal JA. Incidental enchondromas of the knee. AJR Am J Roentgenol 2008;190:1611-5 [Google Scholar] [PubMed]
- 2. Davies AM, Patel A, Azzopardi C, James SL, Botchu R, Jeys L. The influence of site on the incidence and diagnosis of solitary central cartilage tumours of the femur. A 21st century perspective. J Clin Orthop Trauma 2022;32. [Google Scholar] [PubMed]
- 3. Solitary Benign Enchondroma of the Long Bones of the Hand. Available from: https://pubmed.ncbi.nlm.nih.gov/4941379 [Last accessed 2026 Apr 04]. [Google Scholar] [PubMed]
- 4. Kendell SD, Collins MS, Adkins MC, Sundaram M, Unni KK. Radiographic differentiation of enchondroma from low-grade chondrosarcoma in the fibula. Skeletal Radiol 2004;33:458-66. [Google Scholar] [PubMed]
- 5. Geirnaardt MU, Hermans J, Bloem JL, Kroon HM, Pope TL, Taminiau AH, et al. Usefulness of radiography in differentiating enchondroma from central grade I chondrosarcoma. Am J Roentgenol 1997;169:1097-104. [Google Scholar] [PubMed]
- 6. Benign Bone Tumors and Nonneoplastic Conditions Simulating Bone Tumors-Musculoskeletal Key. Available from: https://musculoskeletalkey.com/benign-bone-tumors-and-nonneoplastic-conditions-simulating-bone-tumors [Last accessed on 2026 Apr 24]. [Google Scholar] [PubMed]
- 7. Afonso PD, Isaac A, Villagrán JM. Chondroid tumors as incidental findings and differential diagnosis between enchondromas and low-grade chondrosarcomas. Semin Musculoskelet Radiol 2019;23:3-18. [Google Scholar] [PubMed]
- 8. Goto T, Kawano H, Yamamoto A, Yokokura S, Iijima T, Motoi T, et al. Simple curettage without bone grafting for enchondromas of the foot. Arch Orthop Trauma Surg 2004;124:301-5. [Google Scholar] [PubMed]
- 9. Patil SN, Sandeep S, Ganesh C. Intramedullary enchondroma of distal femur treated with curettage in 31 year old female: A case report. Natl J Clin Orthop 2021;5:93-5. [Google Scholar] [PubMed]
- 10. The Results of Curettage and Bone Cementing for Enchondromas of the Distal Femur – PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/18180573 [Last accessed on 2026 Apr 04]. [Google Scholar] [PubMed]
- 11. Omlor GW, Lohnherr V, Lange J, Gantz S, Mechtersheimer G, Merle C, et al. Outcome of conservative and surgical treatment of enchondromas and atypical cartilaginous tumors of the long bones: Retrospective analysis of 228 patients. BMC Musculoskelet Disord 2019;20:134. [Google Scholar] [PubMed]
- 12. Enchondroma and Chondrosarcoma of Bone: Clinical, Radiologic, and Histologic Differentiation – PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/15116654 [Last accessed on 2026 Apr 04]. [Google Scholar] [PubMed]
- 13. Tuli SM. Turek’s orthopaedics – principles and their applications (7th Edition). Indian J Orthop 2017;51:483. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report
July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report
July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report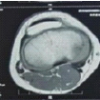 June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum
June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma
June 1, 2026 Atypical Bilateral Cystic Foot Swellings with Osteomyelitis-Like Features: A Diagnostic Dilemma