
Comprehensive anatomical knowledge and understanding of neglected clubfoot is crucial for precise surgical planning.
P K Sankaran, Department of Anatomy, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: drpks@live.com
Abstract
Introduction: Congenital talipes equinovarus is a musculoskeletal deformity causing foot disability with a plantar flexed, inverted and adducted foot. The deformities associated with clubfoot must be corrected at an early age to prevent long-term residual disabilities.
Case Report: In this case, we describe a rare anatomical variation of the neglected adult clubfoot, which was noticed during routine dissection of the lower limb for MBBS at AIIMS, Mangalagiri. The adult neglected clubfoot was dissected to identify the exact soft tissue and bony abnormalities involved in the deformity. The plantar fascia, long flexor tendons of the foot, ligaments of tarsal joints and thick fibrous aponeurotic sheaths were taut, and causing the deformity was identified. The talar head was displaced medially, subluxating the navicular and cuboid, inferiorly misaligning the talocalcaneonavicular joint and calcaneocuboid joint. In addition, deep arches of the foot were prominent with stout metatarsals in a fixed hyperextended deformity.
Conclusion: The knowledge about the bony and soft-tissue abnormalities can be helpful for an orthopaedician in the surgical correction of clubfoot in adults, and they can take precautions in preventing relapse as it requires soft-tissue releases, tendon lengthening procedures, and osteotomies in neglected clubfoot.
Keywords: Clubfoot, cadaveric dissection, neglected clubfoot, foot deformity.
Clubfoot is a congenital deformity that is defined as the inward twisting of the foot, resulting in plantar flexion, inversion, and adduction of the foot. Clubfoot is one of the most common congenital musculoskeletal deformities, with an incidence of approximately one in every 1000 live births globally [1,2]. Clubfoot can occur as an isolated defect, be idiopathic, or be secondary to another neuromuscular condition. The process in which clubfoot develops is still under investigation, but it is a multifactorial process under the influence of genetic and environmental factors that drive the development of abnormal bone, muscle, tendon, and ligaments in the foot [3]. Genetic susceptibility appears to play a substantial role in clubfoot, as demonstrated by an increased incidence in families with a history of clubfoot [4]. Environmental factors during foetal development have also been reported, such as abnormal neuromuscular development, in utero positioning of the foetus, or vascular disturbance during development, which also appears to contribute to the malformation of clubfoot. An abnormality in the development of the muscles, tendons, and ligaments which stabilise the foot will contribute to establishing the inward twisting position known as ‘clubfoot’ [5]. Early treatments for infants with clubfoot deformities are critical to avoid long-term disability and enhance functional outcomes for children affected by clubfoot. The Ponseti non-surgical casting protocol is widely accepted to correct the foot position. In cases that do not respond adequately to conservative treatment or in recurrent deformities, surgical intervention may be required to release tight tendons and correct bone alignment [6]. With appropriate treatment, most individuals with clubfoot can achieve a normal range of motion and engage in typical physical activities, and without any treatment, it will lead to neglected clubfoot and further complications [7,8]. Reviewing the cadaveric details of abandoned clubfoot cases can provide insight into anatomical structure or surgical considerations that may develop for individuals who present in adulthood. These anatomical changes can provide information to surgeons to improve surgical precision and outcomes in neglected or recurrent cases of clubfoot, which can improve individuals’ overall function and quality of life.
During routine First MBBS dissection of the lower limb (LL) in a 55-year-old male cadaver, the right LL was shorter than the left LL, and the right foot was pointed downwards in a plantar flexed position, and the sole was facing an inverted position (Fig. 1a).
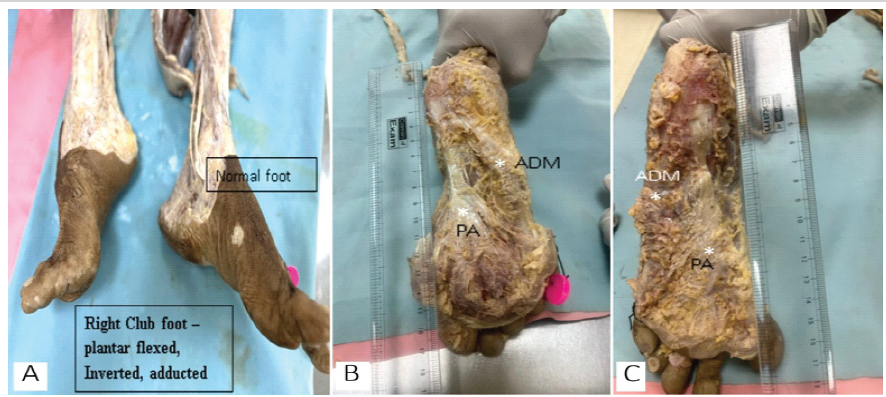
Figure 1: Anatomical abnormalities in a neglected adult talipes equinovarus foot. (a) Plantar-flexed, inverted, and adducted right foot with shortened limb length. (b and c) Shortened right foot length with a thick, taut plantar aponeurosis. The abductor digiti minimi exhibits a thick fibrous aponeurosis, while its muscle belly remains distinct.
It also showed atrophy in left upper limb muscles and also the absence of the pectoralis major with a prominent pectoralis minor, and the thoracic cage was asymmetrical with the right lung completely collapsed with fibrosis. The right calf was small, and the right tendocalcaneus was contracted in length and width and taut with a smaller muscle belly than the left (Fig. 2).
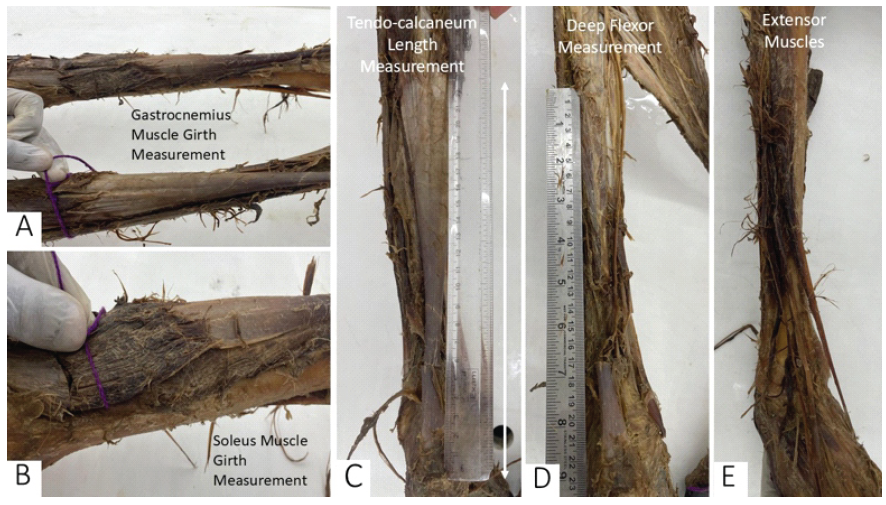
Figure 2: Muscle girth and tendon measurements in a neglected adult talipes equinovarus limb. (a) Measurement of the muscle girth of the gastrocnemius, highlighting muscle atrophy in the affected limb. (b) Measurement of the soleus muscle girth with the gastrocnemius intact, demonstrating relative muscle bulk. (c) Measurement of the length of the tendocalcaneus, emphasizing its shortening and tautness. (d) Dissection of the deep flexor muscles of the leg, revealing structural abnormalities in the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. (e) Extensor muscles of the leg, showing thickened and taut tendons contributing to restricted dorsiflexion in the affected foot.
The muscle bellies of tibialis posterior (TP), flexor hallucis longus (FHL), and flexor digitorum longus were smaller than the left. The flexor retinaculum was normally placed and attached with normal tendon arrangements. There was limited passive dorsiflexion with a thick extensor retinaculum holding the extensor tendons in heightened tension, further restricting the range of motion in the affected foot. In the sole of the foot, the plantar aponeurosis (PA) was a thick band of fibrous tissue with marked shortening and increased tension (Fig. 1b). This tightness may likely contribute to the high arch commonly associated with this foot anomaly. The affected foot has PA, which is 1 cm shorter than that of a normal foot. There was a distinctive thick fibrous band extending from the lateral tubercle of the calcaneum to the fifth metatarsal bone (Fig. 1b), superficial to the abductor digiti minimi (ADM), and this band appears to be a thickened aponeurosis of the ADM and may play a role in the abnormal deep cavus arch of the foot and positioning of the bones and joints in this anomaly; on the left side, the ADM is more of a muscle belly and becomes a tendon near the insertion (Fig. 1c). Deep to that fibrous aponeurosis and lateral to the calcaneum there was a blind bony cavity extending deep up to the lateral malleolus and filled with fat (Fig. 3a). There was also a fibrous arched sheath extending from the medial tubercle of the calcaneum to the navicular bone, the base of the first metatarsal and the abductor hallucis muscle (Fig. 3b and d). The FHL tendon in the foot was extremely taut with a considerable gap filled with fat between skeleton of the foot and the tendon, with an appearance of a string of a bow (Fig. 3c and d). This appearance was holding the foot in a characteristic inversion and adduction position of this anomaly. The peroneus longus (PL) muscle in the foot, after inserting into the cuboid laterally, continued to the base of the first metatarsal for insertion in an extremely taut position (Fig. 3d). The long plantar ligaments, Figs. 3b and 4a, which provide support to the arch, were reduced in length compared to the left, and this may contribute to the rigidity and immobility of the foot.
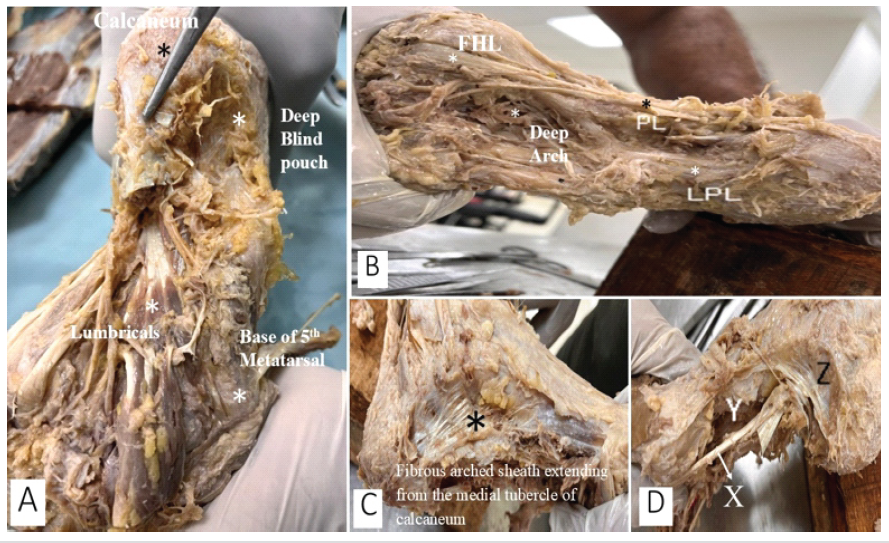
Figure 3: Anatomical structures in a neglected adult talipes equinovarus dissected foot. (a) A deep blind pouch filled with fat is located lateral to the calcaneum and posterior to the base of the fifth metatarsal bone, with blood vessels, nerves, and muscles crowded within the narrow arch of the foot. (b) A fibrous sheath extends from the medial tubercle of the calcaneum to the navicular bone, base of the first metatarsal, and continues with the abductor hallucis. (c) The flexor hallucis longus (FHL) tendon is taut, curving, and crossing the prominent base of the first metatarsal before inserting into the great toe. The peroneus longus enters the sole, inserting into the cuboid and extending as a thick tendon to the base of the first metatarsal, contributing to exaggerated arching by holding the foot’s skeleton tight from lateral to medial. LPL-Long plantar ligament. (d) The sole of the foot exhibits a taut FHL tendon (X) resembling a bowstring, with considerable space filled with fat (Y) deep to it. The arched fibrous sheath extending from the medial tubercle of the calcaneum to the first metatarsus is also visible (Z).
The right foot exhibited a deep cavus arch due to tight ligaments and muscle tendons. The right metatarsal heads, particularly the heads of the first and second metatarsals, were prominent in this specimen, appearing to be a major direct contact in weight-bearing (Fig. 4a and b). This prominence may result from alterations in the alignment and positioning of the metatarsal bones characteristic of this deformity. The navicular has subluxated inferiorly from the talus head, and the cuboid is displaced inferiorly from the calcaneum (Fig. 4c and d), resulting in an inversion deformity.
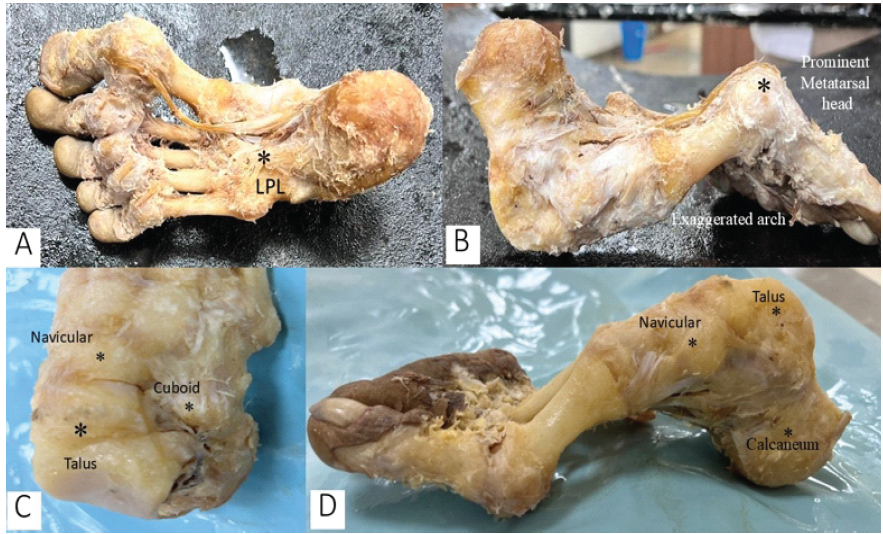
Figure 4: Skeletal abnormalities in a neglected adult talipes equinovarus foot. (a) Foot skeleton with all soft-tissues removed, revealing exaggerated medial, lateral, and transverse arches, along with a prominent first metatarsal head, which serves as the primary weight-bearing point. The long plantar ligaments, extending from the calcaneum to the base of the lateral metatarsals, appear shortened. (b) Foot skeleton in an upside-down orientation, highlighting the deep exaggerated arches and prominent metatarsal heads. (c and d) Subluxation of the talus medially from the navicular (N) bone and displacement of the cuboid from the calcaneum, contributing to the characteristic deformity of the foot.
This study presents a comprehensive cadaveric dissection of an adult case of neglected talipes equinovarus (TEV), examining the anatomical abnormalities at multiple levels, including fascia, ligaments, muscles, tendons, bones, and joints. The findings highlight shortened PA, thickened fibrous bands, contracted tendons, and malpositioned tarsal bones, all contributing to the rigid deformity characteristic of TEV. These observations provide significant insights into the structural pathology of long-standing, untreated clubfoot, which is crucial for understanding its progression and for optimising surgical interventions. The anatomical findings were listed in Table 1.
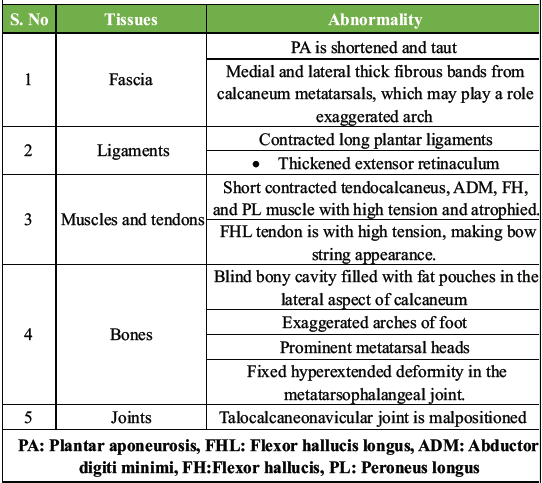
Table 1: Structural abnormalities of foot tissues in club foot
Bony and muscular defects:
The anatomical defects involving bones and soft tissues lead to malpositioned tarsal bones, muscle atrophy, and leg shortening with a characteristic position of the foot [9]. There are lots of studies done on these factors in stillborn and newborn foetuses to explain the patho-anatomical cause for the defect. There are alterations in the development of tarsal bones in terms of their shape and size with their articular relationships with each other in stillbirth foetuses, causing idiopathic congenital clubfoot [10]. This dissection of an adult cadaveric clubfoot (around 60 years old) revealed significant malpositioning of the talus, calcaneum, and navicular bones, affecting the talocalcaneal and talonavicular joint axes. The talus was plantarflexed, with its neck deviated medially, forcing the calcaneum into inversion and adduction. This abnormal bone positioning is well-documented in foetal and infant cadaveric studies, where similar findings have been reported as primary contributors to the structural rigidity of clubfoot [11]. During the correction of the neglected club foot by everting, the calcaneum will compress the anterior aspect against the talus, and only by abducting the calcaneum can the deformity be completely corrected [12]. In the forefoot, the metatarsal heads were so prominent since they are the weight-bearing points, and this has led to stout, thick metatarsals and exaggerated the arches of the feet deeper. In addition, shortened and atrophic muscle bellies of TP, FHL, and PL were observed, with their tendons appearing taut and fibrotic. Prior research has indicated that the severity of clubfoot is inversely proportional to muscle fibre length, as shorter fibres lead to increased collagen deposition and fibrosis, reducing flexibility [13]. In agreement with these studies, our findings suggest that the chronic shortening of tendons fixes the foot in an adducted and inverted position, reinforcing the structural rigidity of neglected TEV. The severity of the clubfoot is inversely proportional to the length of the muscle fibres and tendons; as a result, any tendon-lengthening procedure can replace muscle fibre with excess collagen, leading to relapse within a few years of surgery [14].
Joint and ligament defects:
This dissection highlighted a misaligned talocalcaneonavicular joint, subluxation of the navicular bone inferiorly from the talar head, and inferior displacement of the cuboid from the calcaneum. These joint alterations, combined with taut long plantar ligaments, contributed to the fixed inversion and adduction deformity. Similarly, a study conducted on stillbirth foetuses showed findings with taut long and short plantar ligaments, the tibionavicular (deltoid) ligament, and calcaneonavicular (spring) ligaments. Previous literature supports these findings, showing that chronic misalignment of these joints leads to contractures of associated soft tissues, making correction through conservative means more difficult [15]. The thickened extensor retinaculum observed in this case further restricted dorsiflexion, exacerbating the equinus deformity. The importance of the extensor retinaculum in restricting dorsiflexion has been emphasised in previous studies, with surgical release of this structure recommended in cases of relapsed clubfoot [16]. This malorientation of the articular facets in the talocalcaneo-navicular joints in the neglected clubfoot cannot be corrected accurately using surgery but can be minimised using serial manipulations and castings, normalising the talar neck and navicular articular surfaces [17]. The fusion of joints like talonavicular, calcaneocuboid, and talus with the medial cuneiform was performed using internal fixations with lateral release of fibrous tissue and plantar ligaments in neglected club foot can result in a normal plantigrade foot [18].
Aponeurotic and fascial defects:
The shortened and thickened PA played a major role in sustaining the deep cavus deformity, leading to prominent metatarsal heads as the primary weight-bearing points. A distinctive fibrous band extending from the lateral tubercle of the calcaneum to the fifth metatarsal was observed, which may represent a thickened aponeurosis of the ADM, potentially worsening the exaggerated arch deformity. Such fibrous bands have not been previously reported in TEV literature, making this an important novel observation. In addition, a blind bony cavity lateral to the anterior calcaneum filled with fat was noted, possibly resulting from long-standing abnormal forces on the calcaneocuboid joint. This osseous abnormality has not been described in previous TEV studies and may represent a compensatory response to chronic mechanical stress. The maldevelopment of the talocalcaneo-navicular joint and calcaneo-cuboid joint occurs due to ossification of misaligned bones exposed to abnormal external forces, leading to abnormal bony anatomy [19]. The foot shape cannot be restored when fully ossified in a neglected club foot, and it mostly requires osteotomy surgeries for correcting the defect [20].
Surgical implications:
Our findings reinforce the need for extensive soft-tissue releases, tendon lengthening procedures, and, in severe cases, osteotomies for correction of neglected TEV. Prior studies have shown that Ponseti casting is effective for early clubfoot management, but in neglected adult cases, surgical intervention becomes necessary [21]. The shortened and taut tendons identified in this study highlight the need for Achilles tenotomy, TP lengthening, and lateral column lengthening procedures in the surgical management of severe TEV cases. The role of medial and lateral fibrous aponeurotic bands in maintaining the cavus deformity suggests that plantar fasciotomy and release of these bands should be considered in surgical correction. In addition, the deep-seated osseous abnormalities identified emphasise the potential need for wedge resections of tarsal bones in rigid, neglected cases, a technique supported by recent surgical literature [22]. In neglected adults clubfoot correction requires extensive soft-tissue releases with wedge resection of bones involved and fusion of certain tarsal joints so that the affected foot should be normal-appearing with plantigrade movements. However, the residual deformities like forefoot adducted, valgus ankle, and <10% of heel varus/valgus are acceptable; the knowledge of the abnormal soft tissue and bony factors should be corrected appropriately to prevent relapse [23].
Genetic and developmental considerations:
Recent genetic research has identified mutations in PITX1, HOXD, HOXC9, A9, and TP63 genes as contributors to TEV [24]. These genes regulate LL formation, tendon development, and muscle differentiation, explaining the muscular atrophy and abnormal skeletal positioning observed in this case. In addition, altered DNA methylation patterns and chromosomal variations at 17q23 have been linked to increased clubfoot susceptibility [25]. Furthermore, epigenetic changes in the patterns of DNA methylation can later contribute to clubfoot [26]. A combination of genetic and environmental factors may contribute to TEV pathogenesis.
Strengths of the study:
- Detailed cadaveric analysis of a neglected, adult TEV case provides insights into the long-term effects of untreated clubfoot
- Identification of novel fibrous bands and deep osseous cavities, which have not been previously documented in TEV literature
- Correlation of anatomical findings with genetic studies, offering a developmental perspective on TEV pathology
- Inclusion of high-resolution images demonstrating key anatomical abnormalities, enhancing the clinical applicability of the findings.
Limitations of the study:
- A single cadaveric specimen limits generality; additional cases are needed to confirm findings
- Lack of histological analysis of fibrous tissue, which could further elucidate the composition and pathology of the observed contractures
- Inability to assess the functional biomechanics of the affected limb due to postmortem nature of the study
- Limited discussion of neurovascular components, which may also play a role in TEV progression.
This cadaveric dissection of a neglected adult TEV foot provides critical insights into the structural abnormalities contributing to rigidity due to deformity. The shortened tendons, misaligned joints, and fibrotic soft tissues collectively contribute to the classic TEV presentation. The newly identified fibrous bands and bony cavities highlight previously unreported anatomical changes, emphasising their potential role in TEV pathogenesis. Surgical correction must address all components, such as muscles, tendons, fascia, and bone, to prevent recurrence. Future research should incorporate histological studies, multi-specimen dissections, and biomechanical analyses to further refine our understanding of TEV pathology.
Clubfoot, a prevalent congenital deformity, can lead to lifelong disability and social stigma if left untreated. Timely diagnosis, thorough examination, and informed intervention, grounded in anatomical knowledge, are crucial for effective treatment planning and optimal functional recovery. Orthopaedic surgeons play a vital role in enhancing mobility and quality of life through surgical interventions. By raising awareness and ensuring access to early treatment, we can prevent permanent disability, alleviate healthcare burdens, and promote inclusivity. Early action can significantly improve outcomes, empowering individuals with clubfoot to lead active, fulfilling lives.
References
- 1. Ponseti IV. Treatment of congenital club foot. J Bone Joint Surg Am 1992;74:448-54. [Google Scholar] [PubMed]
- 2. Dobbs MB, Gurnett CA. Update on clubfoot: Etiology and treatment. Clin Orthop Relat Res 2009;467:1146-53. [Google Scholar] [PubMed]
- 3. Ippolito E, Ponseti IV. Congenital club foot in the human fetus. A histological study. J Bone Joint Surg Am 1980;62:8-22. [Google Scholar] [PubMed]
- 4. Wynne-Davies R. Family studies and the cause of congenital club foot. J Med Genet 1965;2:227-32. [Google Scholar] [PubMed]
- 5. Kite JH. Principles involved in the treatment of congenital club-foot. 1939. J Bone Joint Surg Am 2003;85:1847. [Google Scholar] [PubMed]
- 6. Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop 2002;22:517-21. [Google Scholar] [PubMed]
- 7. Zionts LE, Dietz FR. Bracing following correction of idiopathic clubfoot using the Ponseti method. J Am Acad Orthop Surg 2010;18:486-93. [Google Scholar] [PubMed]
- 8. Ippolito E, Gorgolini G. Clubfoot pathology in fetus and pathogenesis. A new pathogenetic theory based on pathology, imaging findings and biomechanics-a narrative review. Ann Transl Med 2021;9:1095. [Google Scholar] [PubMed]
- 9. Windisch G, Anderhuber F, Haldi-Brändle V, Exner GU. Anatomical study for an updated comprehension of clubfoot. Part II: Ligaments, tendons and muscles. J Child Orthop 2007;1:79-85. [Google Scholar] [PubMed]
- 10. Barrie A, Varacallo M. Clubfoot. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 11. Do Amaral E, Peixoto JB, Miyahara LK, Akuri MC, Moriwaki TL, Sato VN, et al. Clubfoot: Congenital talipes equinovarus. Radiographics 2024;44:e230178. [Google Scholar] [PubMed]
- 12. Ponseti IV, Smoley EN. The classic: Congenital club foot: The results of treatment. Clin Orthop Relat Res 2009;467:1133-45. [Google Scholar] [PubMed]
- 13. Dim EM, Edagha IA, Peter AI, Umoh IU, Ituen AM, Dim CO, et al. Congenital talipes equinovarus: A review. J Orthop Surg Tech 2002;5:474-86. [Google Scholar] [PubMed]
- 14. Kadhum M, Lee MH, Czernuszka J, Lavy C. An analysis of the mechanical properties of the ponseti method in clubfoot treatment. Appl Bionics Biomech 2019;2019:4308462. [Google Scholar] [PubMed]
- 15. Riemen A, Lim J, Wong K, Campbell D, Pease FJ, Barker SL. Current understandings in congenital talipes equinovarus. Orthop Trauma 2022;36:295-303. [Google Scholar] [PubMed]
- 16. Mustari MN, Faruk M, Bausat A, Fikry A. Congenital talipes equinovarus: A literature review. Ann Med Surg (Lond) 2022;81:104394. [Google Scholar] [PubMed]
- 17. Howard CB, Benson MK. Clubfoot: Its pathological anatomy. J Pediatr Orthop 1993;13:654-9. [Google Scholar] [PubMed]
- 18. Sobel E, Giorgini R, Velez Z. Surgical correction of adult neglected clubfoot: Three case histories. J Foot Ankle Surg 1996;35:27-38. [Google Scholar] [PubMed]
- 19. Windisch G, Anderhuber F, Haldi-Brändle V, Exner GU. Anatomical study for an update comprehension of clubfoot. Part I: Bones and joints. J Child Orthop 2007;1:69-77. [Google Scholar] [PubMed]
- 20. Eidelman M, Kotlarsky P, Herzenberg JE. Treatment of relapsed, residual and neglected clubfoot: Adjunctive surgery. J Child Orthop 2019;13:293-303. [Google Scholar] [PubMed]
- 21. Palmanovich E, Ip W, Em H, Spanko J, Nyska M, Lehnert B, et al. Promising results in a 3-year follow-up for adults undergoing a one-stage surgery for residual talipes equinovarus as part of a humanitarian mission in Vietnam. J Orthop Surg Res 2022;17:493. [Google Scholar] [PubMed]
- 22. Butt MN, Perveen W, Ciongradi CI, Alexe DI, Marryam M, Khalid L, et al. Outcomes of the ponseti technique in different types of clubfoot-a single center retrospective analysis. Children (Basel) 2023;10:1340. [Google Scholar] [PubMed]
- 23. Nordin S, Aidura M, Razak S, Faisham W. Controversies in congenital clubfoot: Literature review. Malays J Med Sci 2002;9:34-40. [Google Scholar] [PubMed]
- 24. Naseem Khan Y, Mahmud MI. Exploring the genetic and pathobiological pathways of talipes equinovarus: A short narrative review. Ital J Anat Embryol 2024;128:25-33. [Google Scholar] [PubMed]
- 25. Xie X, Huang B, Su L, Cai M, Chen Y, Wu X, et al. Prenatal diagnosis and genetic etiology analysis of talipes equinovarus by chromosomal microarray analysis. BMC Med Genomics 2023;16:298. [Google Scholar] [PubMed]
- 26. Yong BC, Xun FX, Zhao LJ, Deng HW, Xu HW. A systematic review of association studies of common variants associated with idiopathic congenital talipes equinovarus (ICTEV) in humans in the past 30 years. Springerplus 2016;5:896 [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Comprehensive Analysis and Surgical Management of Neglected Congenital Talipes Equinovarus Using the Joshi’s External Stabilizing System: A 3-Year Longitudinal Case Study and Biomechanical Review
July 1, 2026 Comprehensive Analysis and Surgical Management of Neglected Congenital Talipes Equinovarus Using the Joshi’s External Stabilizing System: A 3-Year Longitudinal Case Study and Biomechanical Review June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study
June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study May 1, 2026 Reconstructive Surgery for Foot Ectrodactyly in an Adolescent Patient: A Case Report
May 1, 2026 Reconstructive Surgery for Foot Ectrodactyly in an Adolescent Patient: A Case Report March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method
March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method