
Proning is an advanced and common technique in patients requiring ventilatory support. Care should be taken to prevent unrecognised musculoskeletal and neurological injury to the shoulder in the process.
Senthil Muthian, Department of Orthopaedics, Royal Bournemouth Hospital, Castle Lane East, Bournemouth, Dorset BH7 7DW, United Kingdom. E-mail: s.muthian@nhs.net
Abstract
Background: Prolonged proning is widely used in the management of severe acute respiratory distress syndrome (ARDS), most notably during the COVID-19 pandemic. Although brachial plexus injuries are recognised complications, structural shoulder injuries remain rarely reported.
Case Report: We report a case of a patient who developed a glenoid fracture and persistent shoulder dysfunction following prolonged proning for COVID-19-related ARDS. Clinical assessment, radiological findings, and management strategies are detailed.
Discussion: This case highlights unique mechanical and physiological risk factors for structural shoulder injury during proning, including obesity, diabetic neuropathy, prolonged intensive care unit stay, and positioning-related stress.
Conclusion: Structural glenohumeral injuries should be considered in patients presenting persistent shoulder dysfunction after prolonged proning. Awareness and preventive positioning strategies are essential.
Keywords: Proning, brachial plexus injury, acute respiratory distress syndrome, COVID-19, shoulder injury, glenoid fracture.
The long-term health and outcomes of COVID-19 survivors remain incompletely understood. Persistent symptoms have been reported in 40–90% of patients suffering from acute COVID-19 illness. This has been termed post-acute COVID syndrome or “long COVID”. Although the vast majority of persistent symptoms relate to the respiratory system, symptoms include worsening co-morbidities or conditions related to treatment or non-specific symptoms, such as chronic fatigue. We discuss injuries in the shoulder, which can occur as a result of proning, and present a case of shoulder injury sustained during the process of proning, which is a technique used in intensive care patients on ventilator support that helps improve ventilation. The effect of the prone position on causing traction injury to the brachial plexus is well documented from multiple studies predating COVID-19 [1]. To our knowledge, this is the first known case of structural shoulder injury related to proning in the COVID setting. Musculoskeletal complications are increasingly recognised in patients with severe COVID-19, particularly following prolonged intensive care unit (ICU) admission and prone positioning. These include nerve injuries, joint stiffness, and, less commonly, structural shoulder pathology. This case highlights a rare glenohumeral injury occurring in this context, emphasising the need for clinical vigilance [2].
A 58-year-old woman was referred to the orthopaedic unit with persistent left shoulder pain ongoing for 10 months. She had been treated for acute COVID illness at a different hospital, during which time she developed acute respiratory distress syndrome (ARDS), which required ventilation and proning in the ICU for 30 days. She noticed severe shoulder pain during her time in the ICU. She had several co-morbidities, including a high body mass index (BMI) of 40 kg/m2, type 2 diabetes (on metformin), obstructive sleep apnoea (on nocturnal non-invasive ventilation), and cardiac failure. On examination, there was mild tenderness over the left shoulder in the lateral subacromial area and a range of movement of 0–170° forward flexion, 0–170° abduction, 0–70° external rotation, and internal rotation up to L5 actively. Rotator cuff strength was preserved, and impingement and biceps tests were negative. The shoulder was stable. Sensation was reduced in the C5–T1 dermatomes, though there was no obvious motor weakness. Horner’s sign was negative. She had plain radiographs of the shoulder, which were reported as normal (Fig. 1), and a subsequent computed tomography scan of the shoulder was done, which showed an inferior glenoid injury (Fig. 2 and Fig. 3).
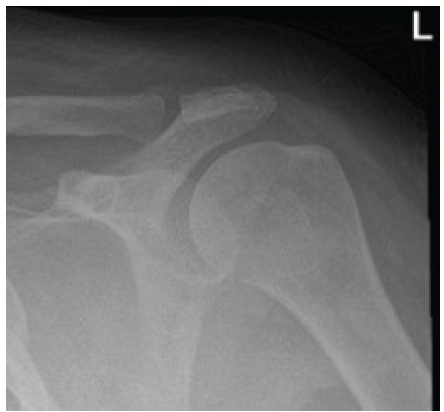
Figure 1: Plain radiograph of the left shoulder.
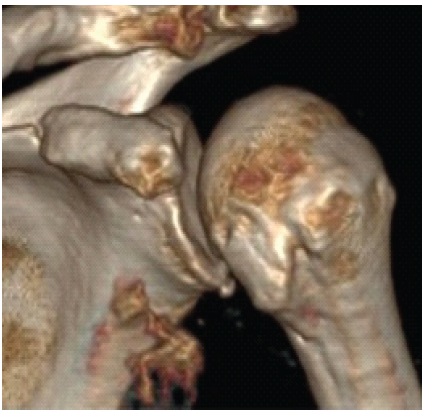
Figure 2: 3D reconstruction computed tomography showing an inferior glenoid fracture.
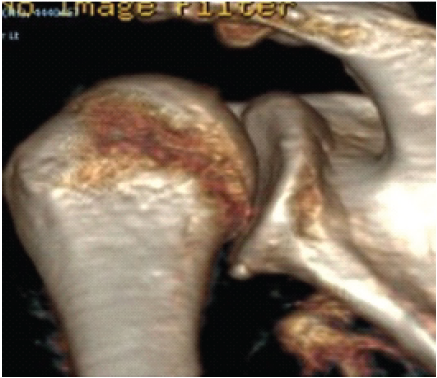
Figure 3: 3D CT scan demonstrating inferior margin of the glenoid
A magnetic resonance imaging arthrogram was subsequently performed and showed an irregular chondral surface with a flap tear of the articular surface near the inferior pole of the glenoid (Fig. 4).
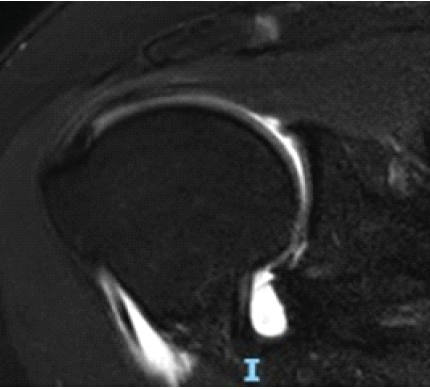
Figure 4: Magnetic resonance imaging arthrogram showing inferior glenoid chondral flap tear. Note the contrast beneath the flap.
She also had a degenerated acromioclavicular joint and an os acromiale, but the glenohumeral ligaments and the rotator cuff were intact. Nerve conduction studies were also performed and revealed no obvious brachial plexus neuropathy, but ulnar nerve compression at the elbow as well as median nerve compression at the wrist, in addition to possible cervical radiculopathy.
Treatment:
The patient was treated non-operatively after a multidisciplinary discussion of all treatment options. She underwent physiotherapy to maintain/improve the range of movement as well as strengthening exercises for the rotator cuff, deltoid, and scapular muscles.
Follow-up:
At 3 months, she reported good improvement, with no pain, and was able to discontinue analgesics. On examination, she was found to have a stable shoulder with a full range of active movement and preserved rotator cuff strength. She was discharged from orthopaedic care.
The use of prone positioning in mechanically ventilated patients with ARDS has been shown to improve oxygenation and reduce mortality from 33% to 16%, particularly during the COVID-19 pandemic [3]. This was done by allowing gravity-assisted drainage of secretions from the posterior aspect of the lungs, allowing alveolar recruitment for gas exchange [4]. In hospitalised patients with COVID-19, 42% developed ARDS, and those patients had a mortality rate of 52% [5]. Despite its respiratory benefits, as shown in this case, proning is associated with a range of musculoskeletal and neurological complications, particularly affecting the upper limbs [6,7]. The present case highlights this, drawing attention to the need for vigilance regarding positioning-related injuries in critical care. Shoulder complications during proning are typically attributed to prolonged traction, compression, and malalignment of the glenohumeral joint or brachial plexus [8]. Commonly reported sequelae include brachial plexus neuropathies, rotator cuff injuries, and subluxations [7,9]. To prevent neural injury, the shoulder should not be positioned in abduction of more than 70° and should be allowed to fall ventrally (to avoid retraction stretching the brachial plexus). The head should be turned slightly toward the arm, which is in abduction, to help protect the brachial plexus, as elongation beyond 10% may cause permanent injury [10]. Clinicians should maintain straight spine alignment and avoid any excessive rotation and avoid extension of the neck. Slide the scapulae up the back with a slight shoulder shrug to avoid depression of the shoulder girdle [8]. Avoid positions of extension of the shoulder or subluxation of the shoulder joint dorsally. The chest should be well supported to ensure the shoulder is forward-flexed. Avoiding abdominal compression is also beneficial in order to reduce venous pressure in the thoracic outlet and neck. Hyperabduction injury of the shoulder girdle resulting in inferior dislocation is usually a high-energy injury associated with a fall where the arm is outstretched and abducted. This results in impaction of the proximal humerus against the acromion, and subsequently the humeral head is levered out of the glenoid socket inferiorly [11]. Direct axial loading with the arm in hyperabduction can also result in inferior dislocation, leading to a bony or chondral injury to the inferior pole of the glenoid. There is an increased incidence of neural injury seen in patients with COVID-19 undergoing ventilation and proning. The reason may be multifactorial, including common risk factors, such as diabetes and obesity. The patient also usually requires a prolonged duration of proning, up to 12 h [7]. Additional contributing factors include a catabolic state and hypoxia. Surgery in the prone position has an increased risk of injury to the brachial plexus due to pressure points or strain in flexion or extension, leading to increased intraneural venous pressure and local oedema [12]. The diagnosis of nerve injury is often delayed, as it is often masked by muscle weakness and debilitation. Shoulder stiffness is another common presentation after an intensive therapy unit. In a study published from Chile on 78 patients undergoing intensive care treatment, 20 were found to have shoulder pain and stiffness. They were assessed and underwent physiotherapy with good outcomes [13]. In a study of 120 patients who received intensive care treatment, 38 patients were referred for formal rehabilitation service, and among them, 18 (47.4%) were found to have persistent shoulder pain and stiffness more than 2 months after discharge [14]. The authors concluded that the risk factors for persistent shoulder pain and stiffness included advanced age, severity of illness, prolonged opioid use, mechanical ventilation for more than 12 days, and ICU stay of more than 15 days. In this case, imaging revealed an inferior glenoid chondral injury with a flap tear, which may have resulted from sustained inferior traction and pressure on the abducted shoulder during repetitive proning cycles. The patient’s high BMI and prolonged proning duration (30 days) are additional risk factors for excessive mechanical load on the shoulder joint. In today’s literature, previous reports have described brachial plexus traction injuries associated with prone positioning, particularly in neurosurgical and spinal procedures where arms are abducted beyond 90° or externally rotated [15]. In critical care settings, especially during the COVID-19 pandemic, these risks may be magnified due to the frequent need for emergency proning, reduced staff ratios, and limited opportunities for repositioning. Although peripheral neuropathies are more frequently documented, structural glenoid or labral injuries, such as the one described here, are rarely reported. This may reflect under-recognition rather than true absence, as shoulder complaints often emerge only after discharge from the ICU. To mitigate these complications, several guidelines recommend meticulous attention to limb positioning during proning. The Intensive Care Society and Faculty of Intensive Care Medicine emphasise alternating arm positions between cycles, avoiding excessive abduction or external rotation, and ensuring adequate padding and support [16]. Regular neurovascular checks and early physiotherapy involvement have also been shown to reduce the incidence of musculoskeletal injuries in ventilated patients. For obese patients or those requiring prolonged proning, additional manual support or the use of proning aids may reduce joint stress. This case underscores the importance of systematic post-proning assessment, particularly in patients who have undergone prolonged mechanical ventilation. Persistent shoulder pain or sensory changes should prompt early imaging to exclude articular or neurogenic causes. As awareness of post-COVID musculoskeletal sequelae grows, integrating structured post-ICU and orthopaedic assessments could improve detection and rehabilitation outcomes for similar injuries. In summary, while proning remains a cornerstone in the management of severe COVID-19-related and non-COVID-19-related ARDS, clinicians should be aware of potential orthopaedic complications as well as known respiratory and systemic complications. Preventative strategies, regular repositioning, and early recognition of shoulder symptoms are essential to avoid long-term morbidity in survivors of intensive care.
The COVID-19 pandemic resulted in a global escalation of patients requiring intensive care and mechanical ventilation, placing significant strain on healthcare resources and manpower. Proning is a proven and efficient technique to improve oxygenation in such patients, gaining prominence during the pandemic and remaining widely used today. Although the pandemic has largely stabilised, proning remains an integral component of modern intensive care practice. This case represents, to our knowledge, the first documented instance of a structural shoulder injury associated with proning in a COVID-19 patient. It highlights the need for continued vigilance in patient positioning and awareness of potential orthopaedic and neurological complications of the practice. Risk factors, such as in this case, obesity, diabetes, increasing age, prolonged ventilation, and multiple co-morbidities, may predispose patients to such injuries. As proning remains a key intervention in managing severe respiratory distress, adherence to established safety protocols and multidisciplinary monitoring is essential to optimise outcomes and minimise preventable harm.
Proning is an advanced technique in patients needing ventilatory support, and care should be taken to prevent unrecognised injury to the shoulder, as described in the first documented case of its kind.
References
- 1. Ball C, Adams J, Boyce S, Robinson P. Clinical guidelines for the use of the prone position in acute respiratory distress syndrome. Intensive Crit Care Nurs 2001;17:94-104. [Google Scholar] [PubMed]
- 2. King-Robson J, Bates E, Sokolov E, Hadden RD. Prone position plexopathy: An avoidable complication of prone positioning for COVID-19 pneumonitis? BMJ Case Rep 2022;15:e243798. [Google Scholar] [PubMed]
- 3. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 2013;368:2159-68. [Google Scholar] [PubMed]
- 4. Koulouras V, Papathanakos G, Papathanasiou A, Nakos G. Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiologic review. World J Crit Care Med 2016;5:121-36. [Google Scholar] [PubMed]
- 5. Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med 2020;180:934-43. [Google Scholar] [PubMed]
- 6. Kwee MM, Ho YH, Rozen WM. The prone position during surgery and its complications: A systematic review and evidence-based guidelines. Int Surg 2015;100:292-303. [Google Scholar] [PubMed]
- 7. Malik GR, Wolfe AR, Soriano R, Rydberg L, Wolfe LF, Deshmukh S, et al. Injury-prone: Peripheral nerve injuries associated with prone positioning for COVID-19-related ARDS. Br J Anaesth 2020;125:e478-80. [Google Scholar] [PubMed]
- 8. Ben-David B, Stahl S. Prognosis of intraoperative brachial plexus injury: a review of 22 cases. Br J Anaesth 1997;79:440-5. [Google Scholar] [PubMed]
- 9. Miller C, O’Sullivan J, Jeffrey J, Power D. Brachial plexus neuropathies during the COVID-19 pandemic: A retrospective case series of 15 patients in critical care. Phys Ther 2021;101:pzaa191. [Google Scholar] [PubMed]
- 10. Simpson AI, Vaghela KR, Brown H, Adams K, Sinisi M, Fox M, et al. Reducing the risk and impact of brachial plexus injury sustained from prone positioning: A clinical commentary. J Intensive Care Med 2020;35:1576-82. [Google Scholar] [PubMed]
- 11. Sheehan SE, Gaviola G, Gordon R, Sacks A, Shi LL, Smith SE. Traumatic shoulder injuries: A force mechanism analysis-glenohumeral dislocation and instability. Am J Roentgenol 2013;201:378-93. [Google Scholar] [PubMed]
- 12. Welch MB, Brummett CM, Welch TD, Tremper KK, Shanks AM, Guglani P, et al. Perioperative peripheral nerve injuries: A retrospective study of 380,680 cases during a 10-year period at a single institution. Anaesthesiology 2009;111:490-7. [Google Scholar] [PubMed]
- 13. Álvarez G, Fernanda Del Valle M, Cordero P, Del Sol M, Lizana P, Gutierrez J. Shoulder pain and stiffness in patients after intensive care unit admission: A prospective study. Rev Chil Reumatol 2021;37:75-81. [Google Scholar] [PubMed]
- 14. Puentez-Gutiérrez JJ, Sánchez-Casado, M.; Díaz-Jiménez, M. Shoulder pain as a residual injury after hospital discharge in patients admitted to the ICU for COVID-19 pneumonia. Med. Clin. (Engl. Ed.) 2021, 156, 301–302. [Google Scholar] [PubMed]
- 15. Yan Y, Bao J, Cai S, Zhong X, Geng B, Liang J, et al. The effects of prolonged prone positioning on response and prognosis in patients with acute respiratory distress syndrome: A retrospective cohort study. J Intensive Care 2025;13:24. [Google Scholar] [PubMed]
- 16. Oliveira VM, Piekala DM, Deponti GN, Batista DC, Minossi SD, Chisté M, et al. Safe prone checklist: Construction and implementation of a tool for performing the prone manoeuvre. Rev Bras Ter Intensiva 2017;29:131-41. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series
July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series May 1, 2026 Arthroscopic Fixation of Acute Reverse Bony Bankart Lesion using Cancellous Cannulated Screws: A Rare Case Report
May 1, 2026 Arthroscopic Fixation of Acute Reverse Bony Bankart Lesion using Cancellous Cannulated Screws: A Rare Case Report April 1, 2026 Multifocal Osteonecrosis in the Hips and Shoulders Bilaterally after Severe COVID-19 Infection Misdiagnosed as Fibromyalgia: A Case Report
April 1, 2026 Multifocal Osteonecrosis in the Hips and Shoulders Bilaterally after Severe COVID-19 Infection Misdiagnosed as Fibromyalgia: A Case Report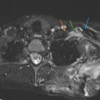 December 1, 2025 Dorsal Claviculectomy For Treatment Of Brachial Plexus Injury After Scapulothoracic Fusion: A Case Report And Literature Review
December 1, 2025 Dorsal Claviculectomy For Treatment Of Brachial Plexus Injury After Scapulothoracic Fusion: A Case Report And Literature Review