
Giant cell tumours of bone should be considered as a differential diagnosis for any lytic lesion, even at uncommon sites, and in treatment, along with adjuvants, bisphosphonates also can be used in decreasing the chances of recurrence.
Dr Rajesh Thakur, Department of Orthopaedics, Tata Main Hospital, Jamshedpur, Jharkhand, India. E-mail: rthakur15@hotmail.com,
Abstract
Introduction: Giant cell tumours of bone are commonly seen in the distal femur, proximal tibia and distal radius and are seen in the age group of 20–40 years with female preponderance. Being close to the joint, the management is formidable, and there are no clinical, radiological or histological parameters to predict chances of recurrence or metastasis. Here, we present a rare case of a giant cell tumour of the distal tibia treated successfully with no recurrence at the end of 4 years.
Case Report: A 33-year-old female presented with complaints of pain, swelling and decreased range of motion (ROM) at the left ankle joint for 6 weeks. On examination, we observed swelling and tenderness in the left ankle joint with decreased ROM. X-rays and computed tomography revealed a well-defined expansile osteolytic lesion in the distal epiphysio-metaphyseal region of the left tibia without a breach in the tibial cortex or ankle joint. Surgery by extensive curettage, adjuvants, cementation and prophylactic fixation was performed. Oral alendronate was started and continued for 24 months after surgery.
Conclusion: The patient at the 4-year follow-up is doing well, walking without pain, able to squat, and having full ROM of the ankle joint with no signs of recurrence.
Keywords: Giant cell tumor of distal tibia, curettage, cementation and fixation, bisphosphonates.
Giant cell tumour of bones (GCTB) is a primary benign but locally aggressive bone tumour, most commonly occurring in long bones of young adults with a female preponderance affecting people aged 20–40 years [1,2]. It accounts for approximately 5% of all primary bone tumours [3]. It is characterised by the presence of large multinucleated osteoclast-like giant cells, facilitating bone destruction [4]. The commonly affected site is around the knee joint, followed by the distal radius [3]. We are here reporting a rare case of GCTB in the lower end of the tibia in a 33-year-old female. The treatment in GCTB is surgical removal, and the surgical options vary from intralesional curettage (IC) to en bloc resection [5]. Preferably, the IC is combined with local adjuvants, including alcohol, phenol, liquid nitrogen, argon beam coagulation, cryo-ablation, hydrogen peroxide and mechanical high-speed burr [2,4,6]. The cavity after IC is usually filled with an autologous or allogenous bone graft or preferably with polymethylmethacrylate cement (PMMA), as PMMA has many advantages over a bone graft [6,7]. Bisphosphonates with anti-osteoclastic activity have been investigated and found to be efficient in controlling disease progression and reducing recurrence [4,8]. The drug is used in pre-operative and post-operative periods for a long duration.
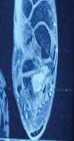
A 33-year-old female presented with pain and swelling at her left ankle for the last 6 weeks after a twisting injury. She first visited another doctor 2 weeks back, but pain persisted. On our evaluation, there was swelling at the anterolateral corner of the left ankle with mild tenderness and painfully decreased range of motion at the left ankle. Ankle radiograph demonstrated a well-defined, radiolucent lesion in the distal tibia anterolaterally extending to subchondral bone. The tibial cortex appeared intact, and the ankle joint was congruent and apparently not breached (Figs. 1 and 2). Computed tomography (CT) of the left ankle revealed an expansile, eccentric osteolytic lesion in the distal tibia with cortical thinning but continuity still maintained and a similarly intact tibio-talar joint surface (Figs. 3 and 4). GCTB was the most probable provisional diagnosis. The patient was planned for an incisional biopsy/frozen section and treatment accordingly as soon as possible. We applied a back slab and started oral alendronate 70 mg/week. She got herself admitted after 4 weeks for the planned surgery. Required blood investigations, chest X-ray and chest CT were done, which were clear. Under spinal anaesthesia and with the patient in the supine position, a tourniquet was applied, and an anterolateral approach to sufficiently expose the tumour site was used. The lesion was curetted a bit, and sampled tissue was sent for a frozen section, which confirmed it as consistent with GCTB. On the confirmation of being benign, we moved as per the treatment plan, which was extensive IC, use of hydrogen peroxide, high-speed burr, cementation and prophylactic fixation with a plate. The distal tibia was considerably exposed with mobilisation of the tendon and neurovascular bundle. A cortical window of good size was made, and extensive curettage beyond the tumour margin into the normal bone was done, carefully preserving the ankle joint line. As an adjuvant, a hydrogen peroxide wash and high-speed burr were used. From a medial approach, a plate with screws was used for prophylactic fixation of the distal tibia, and the screws in the distal tibia were used as rebar to maintain the cement plug. Under fluoroscopic guidance, the big cavity formed after complete resection of the tumour was packed with bone cement. Closure was done, and pressure dressings were completed. The tourniquet was deflated.
Post-operative care and follow-up:
In the immediate post-operative time, limb elevation was done, and the patient was encouraged for active ROM exercises of the ankle after 24 h of surgery. Strict non-weight-bearing for 6 weeks after surgery with physiotherapy. Then, partial weight-bearing with crutches was allowed and full weight-bearing at 12 weeks. Alendronate was advised for 24 months, which she continued. She was back to her office job in 14 weeks after surgery. She gained full ROM of the ankle, pain-free walking and the ability to squat. She was followed for 4 years, and she is doing well. A repeat X-ray at intervals reveals no abnormality or recurrence (Fig. 5 showing radiograph at 6 months and Fig. 6 at 4 years).
GCTB accounts for around 5% of all primary bone tumours [3]. They are expansile, osteolytic, benign but locally aggressive neoplasms but rarely can metastasise (3%) [1,4]. These are commonly seen around the knee and distal radius. Only rarely can they be seen in other sites, such as the distal tibia, as in this case presented here. Involvement of the foot and ankle is rare and comprises <4% of all GCTB [9]. The typical appearance of GCTB is best demonstrated on conventional radiographs, which show a lytic lesion with a geographic type of bone destruction; a well-defined but non-sclerotic margin, eccentric in location, that extends to the subchondral bone; and occurs in patients with closed physis [10]. The abundance of multinucleated osteoclast-like giant cells is a histological hallmark of the tumour which mediates bone destruction [4,5,11]. The tumour tissue contains spindle-shaped stromal cells, which are the primary neoplastic cells [1,4,12]. Their biological behaviour and typical juxta-articular location require specific surgical management with adjuvants. Extensive curettage is the surgical treatment of choice, especially if the cortex is intact and the joint line is not penetrated [2,10,13]. Literature suggests that IC strikes the best balance between controlling disease and preserving function in most of the cases [14]. Chances of recurrence and loss of support of the articular surface have continued to plague the treatment of GCTB. The recurrence rate is nearly 50% with conventional curettage and bone grafting [6]. Surgeons face difficulty in differentiating the radiographic changes seen with the bone graft incorporation and recurrence of the tumour [9]. PMMA is an ideal filler of the cavity created as the cement provides early weight-bearing, early rehabilitation, no donor site morbidity, ease of detection of recurrence, and has a tumouricidal effect by its exothermic reaction, monomer diffusion, and hypoxaemia [9,13]. Bone cement has been proposed to reduce local recurrence, resulting in disease-free survival rates as high as 85% [2]. It was documented that polymethylmethacrylate enhances the margin of the tumour cavity by 1.5–2 mm in cancellous bone and 0.5 mm in cortical bone [6,12]. Local adjuvant therapy with cytotoxic agents like hydrogen peroxide and the use of high-speed burrs have been used intra-lesionally to improve local margins and reduce recurrence [6,10]. In one study, it was recorded that use of cementation, prophylactic fixation, argon laser, and hydrogen peroxide perhaps contributed to no recurrence after 3.5 years [11]. Several other authors have since documented recurrence rates between 8% and 15% using these methods [6,12]. It was seen that the use of prophylactic fixation to stabilise the distal tibia cortex during surgical treatment of GCTB of the distal tibia contributes to the prevention of pathological fracture [11]. Bisphosphonates with an anti-osteoclastic effect were introduced with good efficacy [2]. This drug promotes apoptosis of the stromal cells in GCTB [8,15]. It was found to reduce recurrence after surgery. Balke et al. reported that patients treated with oral alendronate (70 mg/week) for 24–32 months showed that most tumours did not increase in size, and control of recurrence and pain was achieved, and did not report any untoward effects [8].
We must think of the rare occurrence of GCTB in unusual sites, as it is scarcely seen in the distal tibia and demands careful management to have a disease-free and quality life. In the 4 years of follow-up in our case, we observed that extensive IC, adjuvants, cementation and prophylactic fixation supports joint preserving surgery and prevent pathological fracture. Use of bisphosphonates can halt progression of disease and prevent recurrence, and this case, as well few other studies, highlight the need to establish the efficacy of bisphosphonate and inclusion in standardised protocols for the treatment of GCTB.
Giant cell tumours deserve consideration as a differential diagnosis of any lytic bone lesions in young adults. Although they are common at the distal femur, proximal tibia, and distal radius, they can also occur at a rare location like the distal tibia, as seen in our patient. Extensive intralesional curettage, hydrogen peroxide, high-speed burr, cementation, and alendronate give excellent results and reduce the chances of recurrence, and prophylactic fixation prevents pathological fracture.
References
- 1. Sobti A, Agrawal P, Agarwala S, Agarwal M. Giant cell tumour of bone – an overview. Arch Bone Jt Surg. 2016;4:2-9. [Google Scholar] [PubMed]
- 2. Vaishya R, Pokhrel A, Agarwal AK, Vijay V. Current status of bone cementing and bone grafting for giant cell tumours of bone: A systemic review. Ann R Coll Surg Engl 2019;101:79-85. [Google Scholar] [PubMed]
- 3. Mendenhall WM, Zlotecki RA, Scarborough MT, Gibbs CP, Mendenhall NP. Giant Cell Tumour of Bone. Am J Clin Oncol 2006;29:96-9. [Google Scholar] [PubMed]
- 4. Tse LF, Wong KC, Kumta SM, Huang L, Chow TC, Griffith JF. Bisphosphonates reduce local recurrence in extremity giant cell tumours of bone: A case-control study. Bone 2008;42:68-73. [Google Scholar] [PubMed]
- 5. Amri R, Ayedi M, Aifa S, Keskes H. Surgical approaches for the treatment of giant cell tumours of bone in Tunisian patients: Association with recurrence. Libyan J Med 2025;20:2494885. [Google Scholar] [PubMed]
- 6. Gillani SF, Iqbal Y, Taqi M, Ahmad Blouch T, Iqbal M, Siddiq A. Recurrence rate of giant cell tumour with the treatment of scooping curettage, burr-down technique, phenolisation, and bone cement. Cureus 2020;12:e11953. [Google Scholar] [PubMed]
- 7. Persson BM, Ekelund L, Lövdahl R, Gunterberg B. Favourable results of acrylic cementation for giant cell tumours. Acta Orthop Scand 1984;55:209-14. [Google Scholar] [PubMed]
- 8. Balke M, Campanacci L, Gebert C, Picci P, Gibbons M, Taylor R, et al. Bisphosphonate treatment of aggressive primary, recurrent and metastatic giant cell tumour of bone. BMC Cancer 2010;10:462. [Google Scholar] [PubMed]
- 9. Mohapatra AR, Choudhury P, Patel PS, Malhotra RS, Patil AB. An unusual case of a giant cell tumour of the distal tibia. J Orthop Case Rep 2018;8:29-31. [Google Scholar] [PubMed]
- 10. Mavrogenis AF, Igoumenou VG, Megaloikonomos PD, Panagopoulos GN, Papagelopoulos PJ, Soucacos PN. Giant cell tumour of bone revisited. SICOT J 2017;3:54. [Google Scholar] [PubMed]
- 11. Napoli R, Mukherjee A, Rossi M, Distal tibia giant cell tumour surgical treatment: A case report. Foot Ankle Surg Tech Rep Cases 2024;4:100352. [Google Scholar] [PubMed]
- 12. Jha Y, Chaudhary K. Giant cell tumour of bone: A comprehensive review of pathogenesis, diagnosis, and treatment. Cureus 2023;15:e46945. [Google Scholar] [PubMed]
- 13. Medhi M, Badole CM, Mote G. Treatment of giant cell tumours of bone by radical curettage and bone cement. Int J Res Med Sci 2019;7:161-4. [Google Scholar] [PubMed]
- 14. Puri A, Agarwal M. Treatment of giant cell tumours of bone: Current concepts. Indian J Orthop 2007;41:101-8. [Google Scholar] [PubMed]
- 15. Chang SS, Suratwala SJ, Jung KM, Doppelt JD, Zhang HZ, Blaine TA, et al. Bisphosphonates may reduce recurrence in giant cell tumours by inducing apoptosis. Clin Orthop Relat Res 2004;426:103-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report
July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report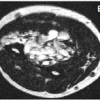 June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review
June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review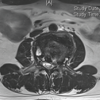 May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report
May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report