
Stabilisation of chronic acromioclavicular joint instability without a tendon graft can provide favourable functional outcomes and may represent a viable alternative to routine tendon graft augmentation.
Andreas Klonz, MD, ATOS Klinik Heidelberg, Bismarckstraße 9–15, 69115 Heidelberg, Germany. E-mail: klonz@sportchirurgie-heidelberg.de
Abstract
Introduction: Chronic acromioclavicular joint (ACJ) instability only rarely causes significant symptoms. In the uncommon cases with substantial pain and impairment, surgical treatment may become necessary. Many surgeons recommend tendon-graft augmentation to reconstruct the coracoclavicular (CC) ligaments. However, it remains unclear whether graft use is mandatory in all chronic cases. This study evaluates clinical and radiographic outcomes after open reduction and stabilisation of chronic ACJ dislocations without grafting.
Materials and Methods: Sixteen consecutive patients with chronic, symptomatic ACJ instability who had initially been managed non-operatively underwent delayed surgical stabilisation without tendon-graft augmentation. After diagnostic arthroscopy, CC stabilisation was performed using a cortical button construct (modified open MINAR® technique). Temporary acromioclavicular (AC) transfixation with two K-wires was added to ensure anatomical reduction, to assist in horizontal stability, and to protect the CC construct during early healing. Thirteen patients were available for clinical and radiographic follow-up. Outcomes included the subjective shoulder value (SSV), ACJ instability score (ACJIS), and Taft score, as well as radiographic assessment of vertical and horizontal alignment.
Results: The mean interval between injury and surgery was 46.5 weeks (range 8–130 weeks). At a mean follow-up of 51 months, mean SSV was 87%, mean ACJIS was 85.5 points, and mean Taft score was 11.1 points. No complications or revision procedures occurred. Some residual vertical or horizontal radiographic displacement was common but did not correlate with inferior clinical outcome.
Conclusion: Open reduction and stabilisation of chronic ACJ dislocations without tendon grafts results in favourable mid-term outcomes comparable to those reported for graft-augmented techniques. Tendon-graft augmentation may not be mandatory in chronic cases, and graft-free reconstruction represents a reasonable option. We believe that adequate preparation of the CC space, anatomical reduction, and rigid fixation are key prerequisites.
Keywords: Chronic instability, acromioclavicular joint, AC-joint, acromioclavicular joint, tendon graft, technique, surgery, minar.
Aim and Background:
Acromioclavicular joint (ACJ) injuries are frequent in young and active individuals and account for a relevant proportion of shoulder girdle trauma [1,2,3]. Lower-grade injuries are generally treated non-operatively, whereas high-grade dislocations are often managed surgically. Despite appropriate initial treatment, few patients develop persistent pain, weakness, scapular dyskinesis, and functional limitation due to chronic instability of the ACJ [3,4]. Chronic ACJ instability is typically defined when the interval between the initial trauma and surgery exceeds several weeks, after which biological healing of the coracoclavicular (CC) ligaments is considered unlikely [4,5]. On this basis, many authors advocate tendon-graft augmentation for anatomical CC reconstruction in chronic cases, aiming to replace the torn tendons and to restore both vertical and horizontal stability [6,7,8,9,10,11]. However, there is no consistent clinical evidence that tendon-graft augmentation is mandatory in all chronic cases. Augmentation increases the complexity of the procedure and is related to a considerable rate of complications such as infection, osteolysis, tunnel widening, and fractures [11,12,13]. Graft harvest may be associated with donor-site morbidity, and several studies have reported residual radiographic displacement even after augmented reconstruction [6,7,8,9,11,13]. Conversely, favourable outcomes have also been described after graft-free techniques in patients with chronic ACJ instability [14,15]. These observations raise the question of whether routine tendon-graft use is really necessary or yields superior results. The purpose of this study was to evaluate the clinical and radiographic outcomes of patients with chronic ACJ instability who underwent secondary surgical stabilisation without tendon-graft augmentation. We hypothesised that graft-free stabilisation would yield favourable mid-term outcomes comparable to those reported for graft-based techniques.
This retrospective observational study included all consecutive patients who underwent surgical treatment for chronic symptomatic ACJ instability between October 2008 and November 2017 at a single orthopaedic institution. The study was approved by the ATOS Institutional Ethics Committee (IEC Number 5/17, November 03, 2017). ‘Chronic instability’ was defined as persistent symptoms after non-operative management and a minimum interval of 8 weeks between injury and surgery, consistent with published thresholds suggesting that intrinsic CC-ligament healing is unlikely beyond this period [4,5]. Patients with low-grade injuries (Rockwood 1), acute ACJ dislocations, associated fractures, prior surgery on the ACJ or on the affected shoulder, or insufficient radiographic documentation were excluded. Sixteen patients met the inclusion criteria. Demographic and injury-related data were collected from medical records. Thirteen patients were available for complete clinical and radiographic follow-up at a minimum of 19 months. All procedures were performed by the senior author. Surgery began with a diagnostic shoulder arthroscopy to exclude and, if necessary, address intra-articular pathology. Subsequently, open debridement of the subacromial space and ACJ region was performed. CC stabilisation was achieved using a cortical button construct comparable to the MINAR® technique [16]. Two transclavicular and one transcoracoid bone tunnels were created, and the suture-button device was secured beneath the coracoid and over the clavicle. To ensure anatomical reduction, to address horizontal instability, and to protect the CC construct during early healing, temporary acromioclavicular (AC) transfixation with two K-wires was added (Fig. 1). The delto-trapezoid fascia was carefully repaired. Post-operative management consisted of sling immobilisation for 3 weeks, followed by passive and active-assisted mobilisation as tolerated. Load-bearing and contact activities were restricted until K-wire removal at 10 weeks. Physiotherapy was continued thereafter to restore motion and strength. Outcome assessment at follow-up included the subjective shoulder value (SSV), the ACJ instability score (ACJIS), and the Taft score [17,18,19,20,21]. The ACJIS and Taft Score were chosen because they are specific to ACJ pathology and, therefore, considered more appropriate for this indication than general shoulder scores. Radiographic assessment consisted of bilateral panoramic stress views (Fig. 2) and Alexander views to evaluate vertical and horizontal alignment [14,15,22]. Due to the small sample size and observational study design, the statistical analysis was descriptive. Continuous variables were summarised as mean, standard deviation (SD), and range.
Sixteen consecutive patients met the inclusion criteria and underwent graft-free stabilisation for chronic ACJ instability. All patients had persistent symptoms despite an initial period of non-operative treatment and fulfilled the predefined interval between injury and surgery. At the time of follow-up, 13 of the 16 operated patients were available for complete clinical and radiographic assessment, corresponding to a follow-up rate of just over eighty per cent (1 × Rockwood II, 6 × Rockwood III, 6 × Rockwood V). Three patients could not be re-evaluated. Reasons for the loss of follow-up in three cases were, in one, a psychiatric illness, and in two cases, the journey for examination was too far. The latter two were interviewed by telephone and reported subjective satisfaction with the surgically treated ACJ. Functional and radiographic scores were not recorded in these cases; only the SSV was recorded. The mean interval between the initial injury and surgical stabilisation was 46.5 weeks (range 8–130 weeks). At the time of surgery, all patients reported relevant pain and functional limitation of the shoulder, particularly with overhead activities and loading in the horizontal plane. At a mean follow-up of 51 months (range, 19–84 months), the clinical results were generally favourable. The SSV averaged 87%, with individual scores ranging from 60% to 100%. Thus, most patients judged the operated shoulder to function at least four-fifths as well as the contralateral side, and several perceived almost normal function. The mean ACJIS was a total of 85.5 points. The pain subscore indicated low levels of residual pain, with a mean score of 18.75 points (SD = 3.0) out of a maximum of 20 points, good performance in activities of daily living (10; SD = 0; max = 10), and high ratings for shoulder strength and overall function (10; SD = 0; max = 10). Cosmetic appearance of the shoulder region was also rated positively by most patients (7.5; SD = 4.0; max = 10). Strength was rated 15 (SD = 3.4; max = 15). The mean Taft Score was 11.1 points, with favourable values in the domains of pain (3.7 points; SD = 0.7; max = 4), strength (3.8; SD = 0.6; max = 4), and radiographic appearance (3.5; SD = 0.5; max = 4). Taken together, these findings indicate that the majority of patients experienced substantial clinical improvement after surgery. Radiographic analysis at follow-up demonstrated a stable situation in vertical alignment in most cases (Figure 2). In several patients, a certain degree of residual vertical and/or horizontal displacement of the distal clavicle relative to the acromion was present (ACJIS 28.3 points; SD = 9.5; max = 35) The mean CC distance on the surgically treated side was 11.4 mm (range 8.3–11.4; SD = 2.2) and on the contralateral side 9.9 mm (range 7.6–13.0; SD = 1.7). In seven cases, the lateral clavicle was stable with the acromion and a vertical translation of <10%. Four patients showed a difference in ACJ alignment of 10–25%. A vertical instability with a difference to the contralateral side of the ACJ alignment of 25–100% was observed in 2 cases. The evaluation of the horizontal instability was performed using the Alexander-view with horizontal adduction of the arm. Eight patients (61.5%) showed stable ACJ. In one case (7.7%), a dislocation of less than one clavicle shaft width was observed. A dislocation of more than the width of the shaft was observed in 4 patients (30.8%). However, patients with such residual displacement did not report worse pain or function, and their clinical scores did not differ meaningfully from those with more anatomical alignment. From a clinical perspective, residual malalignment on static radiographs therefore did not appear to be associated with an unsatisfactory outcome in this cohort. No intraoperative or post-operative complications were recorded. In particular, there were no cases of deep infection, neurovascular injury, loss of reduction requiring revision surgery, or hardware failure. Temporary K-wire fixation was removed after the planned period without adverse events. No patient required revision surgery during the follow-up period.
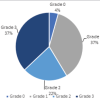
The principal finding of this study is that open reduction of chronic ACJ dislocations with stable 3-dimensional fixation but without tendon grafts provided favourable mid-term outcomes, with high patient satisfaction and an absence of complications or revision procedures. These results demonstrate that satisfactory clinical outcomes may be achieved without tendon-graft augmentation, even when the interval between injury and surgery clearly exceeds the usual time frame associated with primary CC-ligament healing [4,5]. Recent meta-analyses [11,12,13] have demonstrated that a variety of surgical techniques are currently used for the treatment of chronic ACJ instability. Nevertheless, there is still no clear evidence favouring one procedure over another, and the overall methodological quality of the available studies remains low. Stabilisation procedures find their origin in the Weaver-Dunn technique. The current standard for surgical addressing of chronic ACJ instabilities without a tendon graft is the implantation of the hook plate. Alternative procedures include synthetic thread/ligament constructions or K-wire stabilisation [4]. The hook-plate presents the highest biomechanical stability due to the static principle and associated rigidity. Various working groups postulated in a small case series that the treatment of chronic ACJ instabilities with a hook plate could be considered based on sufficient results [23]. However, the obligatory removal of the hook plate after healing was described as disadvantageous. Giannotti et al. examined 17 patients after ACJ stabilisation of acute and chronic ACJ instabilities using the LARS ligament and reported sufficient clinical results [24]. DeBerardino et al. described a cortical button technique using an autologous tendon graft for the first time in 2010 and achieved satisfactory results [19]. Mazzocca et al. compared the stability of a tendon graft with the original CC ligaments and showed that an anatomically placed tendon graft has almost the same stability [8]. Measured by biomechanical stability, Costic et al. recommend using the semitendinosus tendon [21]. Tauber et al. compared clinical and radiological results of the modified Weaver-Dunn technique in chronic ACJ instabilities with the implantation of the semitendinosus tendon combined with a cortical button in the sense of a single bundle technique. Here, the stability with the semitendinosus tendon was superior to the modified Weaver-Dunn technique [1]. Spencer et al. examined X-rays in 154 cases after ACJ stabilisation in chronic ACJ instability in a retrospective review and compared four different surgical techniques with regard to postoperative stability. Here, a post-operative loss of reduction resulted in 21.4%. The use of an allograft loop around the coracoid combined with cortical endobutton fixation showed the lowest failure rate [22]. Further studies show advantages of a triple-bundle stabilisation. The tendon graft replaces not only the CC ligaments but also the AC ligament. Tauber et al. showed results of this technique in chronic ACJ instabilities using an autologous semitendinosus tendon (n = 12). A statistically significant higher horizontal ACJ stability was observed compared to the single bundle technique (n = 14). Score results showed 84.7 P in the ACJIS, 10.9 P in the TS, and an SSV of 84.1% in the triple bundle group. In this group, a posterior subluxation of the lateral clavicle was observed in 25%, compared to a posterior instability of 71% in the single bundle group [7]. Slightly better results were reported by Kraus et al. using arthroscopic CC and AC graft augmentation in 14 patients [10] (Graph 1). Jensen et al. also showed satisfactory results after CC band augmentation using autologous gracilis tendon and additive AC ligament augmentation in chronic ACJ instability. In the follow-up examination, however, no radiological examination was performed, and only sonography was used for imaging, so the results are limited to the TS only [25]. The results with tendon graft in the series of Tauber [7], Kraus [10], and Jensen [25] were comparable to our results without tendon graft and are shown in Graph 1. Cano-Martínez et al. described even better results than Tauber or Jensen in 21 chronic cases that were also stabilised without a graft in a similar technique compared to ours [15]. Borbas in a meta-analysis reported only slightly superior results when tendon grafts were used [9]. Most authors have emphasised the importance of anatomical reduction, vertical and horizontal stability, and reconstruction of the deltopectoral fascia in improving clinical outcomes [10,11,15,26,27]. In recent years, tendon-graft augmentation has been widely recommended in chronic ACJ instability because of its theoretical ability to reproduce the anatomy and biomechanical properties of the CC ligaments more closely than more simple stabilisation techniques [6,7,8,9,10,11]. However, consistent clinical superiority of graft-based reconstruction over graft-free techniques has not been demonstrated across the literature. Graft procedures are significantly more complex. A substantial rate of complications such as tunnel widening, fractures of the clavicle or coracoid, or infection has been reported [11,12,13] and may be expected, especially in the hands of less experienced surgeons. Graft harvest may be associated with donor-site morbidity, increased operative time, and higher cost [13,27,28,29]. At least in patients with moderate functional demands, those unwilling to accept donor site symptoms, or in situations where grafts are limited, graft-free techniques may therefore offer a particularly appealing alternative. However, our findings should not be interpreted as an argument against tendon-graft reconstruction in general. Graft-based reconstruction remains an important technique and may be preferable in patients with previous surgery to the ACJ, pronounced horizontal instability, very high functional demands, or selected revision settings. Instead, our results support the view that tendon-graft augmentation should be considered selectively rather than applied as a universal principle for all chronic cases. One aspect frequently discussed in ACJ reconstruction is the relevance of radiographic alignment. Residual vertical or horizontal displacement after reconstruction has been observed in a considerable proportion of patients in the literature, even after anatomic graft-based reconstruction [9,10,11,12,13,22,23,24,25,26,27]. In the present study, some patients also demonstrated radiographic malalignment at follow-up. Importantly, this did not correlate with poor subjective or functional outcomes, meaning that radiographic perfection is not a prerequisite for clinical success. This is consistent with other reports showing that functional improvement, pain relief, and patient satisfaction do not necessarily depend on complete restoration of ACJ anatomy [9,10,11,12,13,17,18,19,20,21,22]. It is possible that enhancement of stability, adaptation of the soft tissues and neuromuscular structures around the shoulder girdle contributes to long-term pain relief, stability, and function, even when some degree of malreduction persists. This study has several limitations. Its retrospective design and relatively small sample size limit the statistical power and generalisability of the findings. In addition, there was no comparison group treated with tendon-graft reconstruction. Objective strength testing was not performed, and horizontal instability was not quantified beyond radiographic measurement. Finally, three patients were lost to follow-up, although no complications were recorded in these cases before loss to follow-up. Despite these limitations, the present study reflects real-world clinical practice and provides mid-term data supporting graft-free stabilisation as a viable treatment option in selected patients with chronic ACJ instability. In summary, this study demonstrates that graft-free stabilisation of chronic ACJ instability can yield favourable mid-term clinical outcomes. It indicates that graft-free stabilisation still represents a reasonable and less invasive alternative that can be considered within the spectrum of available surgical options for chronic ACJ instability.
Stabilisation of chronic ACJ instability without tendon-graft augmentation resulted in satisfactory clinical outcomes and high patient satisfaction at mid-term follow-up. Routine tendon-graft reconstruction cannot be considered mandatory in all chronic cases. In our opinion, adequate preparation of the CC space, anatomical reduction, and rigid fixation are key prerequisites. Further prospective comparative studies are warranted to better define the indications for graft-based versus graft-free techniques.
Tendon-graft augmentation may not be mandatory in all cases of chronic AC-joint instability. Graft-free stabilisation can be a viable option if adequate preparation of the CC space, anatomical reduction, and rigid fixation are achieved.
References
- 1. Tauber M, Gordon K, Koller H, Fox M, Resch H. Semitendinosus tendon graft versus a modified Weaver-Dunn procedure for acromioclavicular joint reconstruction in chronic cases: A prospective comparative study. Am J Sports Med 2009;37:181-90. [Google Scholar] [PubMed]
- 2. Scheibel M, Ifesanya A, Pauly S, Haas NP. Arthroscopically assisted coracoclavicular ligament reconstruction for chronic acromioclavicular joint instability. Arch Orthop Trauma Surg 2008;128:1327-33. [Google Scholar] [PubMed]
- 3. Gumina S, Carbone S, Postacchini F. Scapular dyskinesis and SICK scapula syndrome in patients with chronic type III acromioclavicular dislocation. Arthroscopy 2009;25:40-5. [Google Scholar] [PubMed]
- 4. Flint JH, Wade AM, Giuliani J, Rue JP. Defining the terms acute and chronic in orthopaedic sports injuries: A systematic review. Am J Sports Med 2014;42:235-41. [Google Scholar] [PubMed]
- 5. Rolf O, Hann von Weyhern A, Ewers A, Boehm TD, Gohlke F. Acromioclavicular dislocation Rockwood III-V: Results of early versus delayed surgical treatment. Arch Orthop Trauma Surg 2008;128:1153-7. [Google Scholar] [PubMed]
- 6. Tauber M, Eppel M, Resch H. Acromioclavicular reconstruction using autogenous semitendinosus tendon graft: Results of revision surgery in chronic cases. J Shoulder Elbow Surg 2007;16:429-33. [Google Scholar] [PubMed]
- 7. Tauber M, Valler D, Lichtenberg S, Magosch P, Moroder P, Habermeyer P. Arthroscopic stabilization of chronic acromioclavicular joint dislocations: Triple- versus single-bundle reconstruction. Am J Sports Med 2016;44:482-9. [Google Scholar] [PubMed]
- 8. Mazzocca AD, Santangelo SA, Johnson ST, Rios G, Dumonski ML, Arciero RA. A biomechanical evaluation of an anatomic coracoclavicular ligament reconstruction. Am J Sports Med 2006;34:236-46. [Google Scholar] [PubMed]
- 9. Bascı O, Duymaz B, Erdogdu IN, Mustafa H O. Combined coracoclavicular ligament and transacromial capsule reconstruction for chronic acromioclavicular joint instability: Clinical and radiological outcomes. Acta Orthop Traumatol Turc 2025;59:170-8. [Google Scholar] [PubMed]
- 10. Kraus N, Hann C, Minkus M, Maziak N, Scheibel M. Primary versus revision arthroscopically-assisted acromio- and coracoclavicular stabilization of chronic AC-joint instability. Arch Orthop Trauma Surg 2019;139:1101-9. [Google Scholar] [PubMed]
- 11. Dyrna F, Berthold DP, Feucht MJ, Muench LN, Martetschläger F, Imhoff AB, et al. The importance of biomechanical properties in revision acromioclavicular joint stabilization: A scoping review. Knee Surg Sports Traumatol Arthrosc 2019;27:3844-55. [Google Scholar] [PubMed]
- 12. Sircana G, Saccomanno MF, Mocini F, Campana V, Messinese P, Monteleone A, et al. Anatomic reconstruction of the acromioclavicular joint provides the best functional outcomes in the treatment of chronic instability. Knee Surg Sports Traumatol Arthrosc 2021;29:2237-48. [Google Scholar] [PubMed]
- 13. Postma SC, van Eecke EP, Mertens BJ, Priester-Vink S, van Deurzen DF, van den Bekerom MP, et al. Allograft vs. autograft for chronic acromioclavicular joint instability: A systematic review and meta-analysis of outcomes and complications. JSES Rev Rep Tech 2025;5:865-77. [Google Scholar] [PubMed]
- 14. Borbas P, Churchill J, Ek ET. Surgical management of chronic high-grade AC joint dislocations: A systematic review. J Shoulder Elbow Surg 2019;28:2031-8. [Google Scholar] [PubMed]
- 15. Cano-Martínez JA, Nicolás-Serrano G, Bento-Gerard J, Marín FP, Grau JA, Antón ML. Chronic acromioclavicular dislocations: Multidirectional stabilization without grafting. JSES Int 2020;4:519-31. [Google Scholar] [PubMed]
- 16. Rosslenbroich SB, Schliemann B, Schneider KN, Metzlaff SL, Koesters CA, Weimann A, et al. Minimally invasive coracoclavicular ligament reconstruction with a flip-button technique (MINAR): Clinical and radiological midterm results. Am J Sports Med 2015;43:1751-7. [Google Scholar] [PubMed]
- 17. Taft TN, Wilson FC, Oglesby JW. Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am 1987;69:1045-51. [Google Scholar] [PubMed]
- 18. Gilbart MK, Gerber C. Comparison of the subjective shoulder value and the Constant score. J Shoulder Elbow Surg 2007;16:717-21. [Google Scholar] [PubMed]
- 19. DeBerardino TM, Pensak MJ, Ferreira J, Mazzocca AD. Arthroscopic stabilization of acromioclavicular joint dislocation using the AC graftrope system. J Shoulder Elbow Surg 2010;19:47-52. [Google Scholar] [PubMed]
- 20. Beitzel K, Obopilwe E, Apostolakos J, Cote MP, Russell RP, Charette R, et al. Rotational and translational stability of different methods for direct acromioclavicular ligament repair in anatomic acromioclavicular joint reconstruction. Am J Sports Med 2014;42:2141-8. [Google Scholar] [PubMed]
- 21. Costic RS, Labriola JE, Rodosky MW, Debski RE. Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med 2004;32:1929-36. [Google Scholar] [PubMed]
- 22. Spencer HT, Hsu L, Sodl J, Arianjam A, Yian EH. Radiographic failure and rates of re-operation after acromioclavicular joint reconstruction: A comparison of surgical techniques. Bone Joint J 2016;98-B:512-8. [Google Scholar] [PubMed]
- 23. Boström Windhamre HA, von Heideken JP, Une-Larsson VE, Ekelund AL. Chronic AC dislocation: Weaver-Dunn augmented with PDS-braid vs hook plate. J Shoulder Elbow Surg 2010;19:1040-8. [Google Scholar] [PubMed]
- 24. Giannotti S, Dell’Osso G, Bugelli G, Cazzella N, Guido G. Surgical treatment of AC dislocation with LARS ligament. Eur J Orthop Surg Traumatol 2013;23:873-6. [Google Scholar] [PubMed]
- 25. Jensen G, Katthagen JC, Alvarado L, Lill H, Voigt C. Arthroscopically assisted stabilization of chronic AC-joint instabilities in GraftRope™ technique with an additive horizontal tendon augmentation. Arch Orthop Trauma Surg 2013;133:841-51. [Google Scholar] [PubMed]
- 26. Saier T, Venjakob AJ, Minzlaff P, Föhr P, Lindell F, Imhoff AB, et al. Value of additional acromioclavicular cerclage for horizontal stability in complete acromioclavicular separation: A biomechanical study. Knee Surg Sports Traumatol Arthrosc 2015;23:1498-505. [Google Scholar] [PubMed]
- 27. Ruffilli A, De Fine M, Traina F, Pilla F, Fenga D, Faldini C. Saphenous nerve injury during hamstring tendon harvest. Knee Surg Sports Traumatol Arthrosc 2017;25:3140-5. [Google Scholar] [PubMed]
- 28. Papastergiou SG, Voulgaropoulos H, Mikalef P, Ziogas E, Pappis G, Giannakopoulos I. Injuries to the infrapatellar branch of the saphenous nerve after hamstring harvest. Knee Surg Sports Traumatol Arthrosc 2006;14:789-93. [Google Scholar] [PubMed]
- 29. Armour T, Forwell L, Litchfield R, Kirkley A, Amendola N, Fowler PJ. Isokinetic evaluation after hamstring tendon ACL reconstruction. Am J Sports Med 2004;32:1639-43. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report
May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review
April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review