
Combined curettage, fibular strut grafting, iliac crest cancellous bone grafting, and stable posterior plating provides effective mechanical stability and biological healing for large recurrent humeral simple bone cysts, enabling early mobilization with low recurrence risk.
Dr. Ritesh K Singh, Department of Orthopedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: singhritesh859@gmail.com
Abstract
Introduction: Simple bone cysts, also known as unicameral or solitary bone cysts, are benign, fluid-filled lesions typically found in long bones, particularly in children and adolescents. The size, location, and symptoms of the cyst determine the course of treatment; approaches range from observation and periodic monitoring to surgical intervention.
Case Report: We report a case treated for a humeral simple bone cyst. A 15-year-old female patient has a history of left humerus titanium elastic nailing system (TENS) nailing for midshaft humerus fracture 9 years ago. Single TENS nail removal was done 8 months post-surgery. The patient has a history of blunt trauma to the operative site 3 months ago, following which the patient developed pain and swelling of the left arm. Curettage of the cyst wall followed by non-vascularised fibula strut grafting and iliac crest bone grafting with posterior humerus plating done. Early postoperative mobilisation was started.
Results: Patients demonstrated significant pain reduction and improved range of motion within 6 weeks postoperatively. Radiographic assessments at 3 months showed near complete integration of the grafts, with signs of new bone formation around the surgical site. The alignment of the humerus was maintained, and there were no instances of hardware failure or recurrence of the cyst noted during follow-up.
Conclusion: The above intervention demonstrates an effective approach to restoring structural integrity and promoting healing. This multimodal approach reduces the risk of complications like fractures and recurrence by strengthening the surrounding bone in addition to treating the cyst itself. Continued monitoring and follow-up are essential to assess long-term success and any potential need for further intervention.
Keywords: Simple bone cyst, iliac crest bone grafting, fibular strut graft.
Simple bone cysts (SBCs), also referred to as unicameral or solitary bone cysts, are benign, fluid- filled osteolytic lesions that predominantly occur in the metaphyseal region of long bones in children and adolescents [1,2]. The proximal humerus and proximal femur are the most frequently involved sites, together accounting for approximately 70–80% of cases [3]. Although SBCs are non- neoplastic, they weaken the structural integrity of bone and predispose patients to pathological fractures, deformity, and functional impairment [4]. The exact etiopathogenesis of SBC remains unclear. Proposed mechanisms include venous obstruction with raised intraosseous pressure, synovial inclusion theory, and localized growth plate abnormalities [2,5]. Many SBCs remain asymptomatic and are detected incidentally or following a pathological fracture after trivial trauma [6]. Symptomatic lesions may present with pain, swelling, or restricted joint motion depending on size and anatomical location [7]. Management strategies for SBCs vary widely. Non-operative treatment with observation may be suitable for small, inactive cysts, while minimally invasive techniques such as intralesional steroid injections, autologous bone marrow injections, and decompression procedures have shown variable success rates and relatively high recurrence [3,8,9]. Surgical intervention is generally indicated for large, symptomatic, recurrent cysts or lesions associated with impending or established fractures [6,10]. Curettage with bone grafting remains a commonly employed surgical option; however, cancellous graft alone may not provide adequate mechanical support in large diaphyseal lesions. Structural grafts such as non-vascularized fibular strut grafts provide immediate stability while promoting biological incorporation [11,12]. Supplementation with internal fixation allows early mobilization and reduces the risk of fracture and recurrence [13].
A 15-year-old female presented with complaints of pain and swelling in the left arm for 3 months. The pain was dull aching, gradually progressive, aggravated by activity, and partially relieved by rest and analgesics. There was no history of fever, weight loss, or constitutional symptoms. The patient had a past surgical history of a mid-shaft fracture of the left humerus sustained 9 years earlier, treated with titanium elastic nailing. Implant removal was done 8 months after fracture union, leaving one nail in situ. The patient remained asymptomatic until 3 months before presentation, when she sustained a trivial blunt trauma to the previously operated arm.
Clinical examination:
On examination (Fig. 1), mild diffuse swelling was present over the mid-arm. Localised tenderness was noted without deformity or abnormal mobility. Shoulder and elbow movements were mildly restricted due to pain. Distal neurovascular status was intact.

Figure 1: Clinical image showing diffuse swelling over the mid-diaphyseal region of the arm.
Radiological assessment:
Plain radiographs of the left humerus demonstrated a well-defined, expansile, lytic lesion involving the diaphyseal region with cortical thinning and mild ballooning with one nail in situ (Fig. 2). The lesion had a narrow zone of transition without periosteal reaction or matrix mineralisation, suggestive of a benign cystic lesion (Fig. 2).

Figure 2: X-ray images.
Magnetic resonance imaging (Fig. 3) revealed a uniloculated cystic lesion with homogeneous fluid signal intensity – hypointense on T1-weighted images and hyperintense on T2-weighted images – without septations or soft-tissue extension, consistent with an SBC [2,7]. Given the size of the lesion, symptoms, and risk of pathological fracture, surgical management was planned.

Figure 3: Magnetic resonance imaging images.
Surgical technique:
The patient was positioned in the lateral decubitus position under general anesthesia. A posterior approach to the humerus was used, with careful identification and protection of the radial nerve (Fig. 4). Implant removal failed despite adequate exposure, and the implant was subsequently cut and left in situ. A cortical window was created, and thorough curettage of the cyst wall was performed until healthy bleeding bone was visualized. A non-vascularized fibular strut graft harvested from the ipsilateral leg was contoured (Fig. 4) and inserted to provide structural support. Additional cancellous bone harvested from the iliac crest was packed around the strut graft to enhance osteogenesis (Fig. 4). Stabilization was achieved using a posterior humerus locking compression plate (Fig. 5).
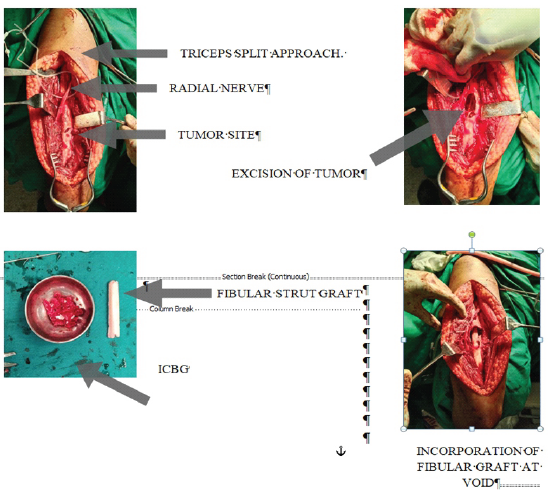
Figure 4: Intraoperative images.
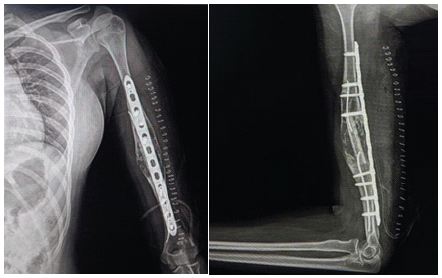
Figure 5: Post-operative X-ray.
Post-operative management and follow-up:
Postoperatively, the limb was supported in a sling. The histopathological report of the specimen sent was suggestive of SBC (Fig. 6). Early passive and active-assisted shoulder and elbow mobilisation was initiated. Progressive strengthening was started after radiological signs of healing. At 6-week follow-up, the patient reported significant pain reduction with improved range of motion (Fig. 7). At 6 months, radiographs showed near-complete graft incorporation with restoration of cortical continuity. There was no loss of alignment, implant failure, or recurrence (Fig. 8).
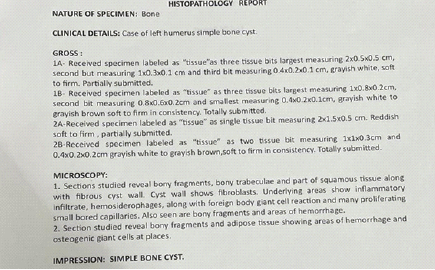
Figure 6: Histopathology report.

Figure 7: Clinical picture.
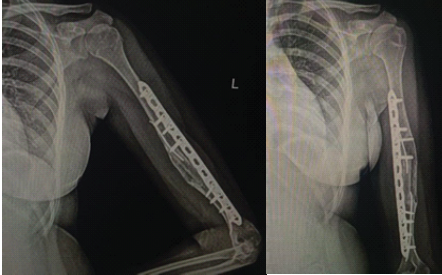
Figure 8: 6-month follow-up.
SBC involving the humeral diaphysis is uncommon and presents a significant therapeutic challenge because of cortical thinning, risk of pathological fracture, and recurrence after inadequate treatment. While minimally invasive methods such as steroid injection, decompression, and bone marrow aspirate injection have shown acceptable outcomes in smaller lesions, larger symptomatic cysts with structural compromise frequently require surgical management [3,8,9]. In the present case, the lesion occurred in a previously operated humerus with retained implant material, making the bone mechanically compromised and biologically altered. Therefore, treatment required not only the eradication of the cyst but also the restoration of structural stability. Thorough curettage remains essential to remove the cyst lining and reduce recurrence [6]. The rationale for using a non-vascularized fibular strut graft was to provide immediate mechanical support to the weakened humeral shaft. Fibular cortical grafts possess excellent compressive strength and act as biological internal splints, particularly useful in diaphyseal defects with cortical thinning [11,12]. In addition, strut grafts help prevent post-operative pathological fracture and maintain alignment until biological incorporation occurs. Recent studies by Shah et al., and Kim et al., demonstrated that fibular strut augmentation in long-bone cystic lesions significantly improves structural stability and facilitates earlier mobilization with lower recurrence rates [14,15,16,17]. However, structural grafts alone have limited osteogenic potential. Therefore, cancellous iliac crest bone graft was additionally used to enhance biological healing. Autologous cancellous graft contains osteogenic cells, osteoinductive growth factors, and an osteoconductive scaffold, thereby accelerating graft incorporation and cortical remodeling [14,18]. The combination of cortical strut support with cancellous grafting provides both mechanical and biological advantages, especially in large cavitary lesions. Rigid fixation using a locking compression plate further enhanced stability and allowed early mobilization. Plate fixation distributes stress across the weakened bone, protects the graft construct, and decreases the likelihood of graft collapse or secondary fracture [13]. Recent literature suggests that combining internal fixation with biological augmentation yields superior functional outcomes in large humeral SBCs compared with grafting alone [17,19]. Another important aspect in this case was the revision nature of surgery. Previous intramedullary fixation and retained implant fragments may have altered local vascularity and biomechanics, potentially contributing to cyst persistence or progression [15]. Despite these challenges, the combined approach achieved excellent radiological incorporation and functional recovery without recurrence at follow-up. Thus, the combination of curettage, fibular strut grafting, cancellous iliac crest grafting, and posterior plating represents a reliable strategy for managing large diaphyseal humeral SBCs, particularly in revision settings where both biological healing and mechanical stability are essential.
Large diaphyseal SBC in young patients requires a comprehensive approach addressing both structural stability and biological healing. Curettage with fibular strut grafting, supplemented by cancellous bone graft and internal fixation, provides reliable outcomes with early rehabilitation and low recurrence rates.
- Large humeral SBCs carry a high risk of pathological fracture
- Structural fibular strut grafting combined with cancellous bone graft and plating ensures both mechanical and biological stability
- Early mobilization leads to superior functional outcomes
Long-term follow-up is essential to monitor healing and recurrence
References
- 1. Neer CS 2nd, Francis KC, Johnston AD, Kiernan HA Jr. Current concepts on the treatment of solitary unicameral bone cyst. J Bone Joint Surg Am 1966;48:731-45. [Google Scholar] [PubMed]
- 2. Wilkins RM. Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-24. [Google Scholar] [PubMed]
- 3. Wright JG, Yandow S, Donaldson S, Marley L, Simple Bone Cyst Trial Group. A randomized clinical trial comparing intralesional bone marrow and steroid injections for simple bone cysts. J Bone Joint Surg Am 2008;90:722-30. [Google Scholar] [PubMed]
- 4. Dormans JP, Pill SG. Simple bone cyst: factors affecting treatment success. J Pediatr Orthop 2002;22:793-8. [Google Scholar] [PubMed]
- 5. Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res 1986;204:25-36. [Google Scholar] [PubMed]
- 6. Capanna R, Campanacci DA, Manfrini M. Unicameral and aneurysmal bone cysts. Orthop Clin North Am 1996;27:605-14. [Google Scholar] [PubMed]
- 7. Spence KF Jr., Bright RW, Fitzgerald SP. Solitary unicameral bone cyst. J Bone Joint Surg Am 1968;50:1485-98. [Google Scholar] [PubMed]
- 8. Scaglietti O, Marchetti PG, Bartolozzi P. The effects of methylprednisolone acetate in the treatment of bone cysts. Results of three years follow-up. J Bone Joint Surg Br. 1979;61-B:200-4. [Google Scholar] [PubMed]
- 9. Chang CH, Stanton RP, Glutting J. Unicameral bone cysts treated by injection of bone marrow or methylprednisolone. Bone Joint Surg Br 2002;84:407-12. [Google Scholar] [PubMed]
- 10. Sung AD, Anderson ME, Zurakowski D, Hornicek FJ, Gebhardt MC. Unicameral bone cyst: A retrospective study of three surgical treatments. Clin Orthop Relat Res 2008;466:2519-26. [Google Scholar] [PubMed]
- 11. Lokiec F, Ezra E, Khermosh O, Wientroub S. Simple bone cysts treated by percutaneous autologous marrow grafting. A preliminary report. J Bone Joint Surg Br 1996;78:934-7. [Google Scholar] [PubMed]
- 12. Cho HS, Oh JH, Kim HS, Kang HG, Lee SH. Unicameral bone cysts: A comparison of injection of steroid and grafting with autologous bone marrow. J Bone Joint Surg Br 2007;89:222-6. [Google Scholar] [PubMed]
- 13. Pogoda P, Linhart W, Priemel M, Rueger JM, Amling M. Clinical relevance of unicameral bone cysts. Arch Orthop Trauma Surg. 2004;124(5):304–8. [Google Scholar] [PubMed]
- 14. Shah H, Patel A, Reddy D, Shah M, Mehta V. Management of large unicameral bone cysts with fibular strut grafting and internal fixation. J Orthop Case Rep 2021;11:45-50. [Google Scholar] [PubMed]
- 15. Kim HS, Park IH, Lee SY, Choi ES, Kim JW. Structural cortical graft augmentation for long-bone cystic lesions: Functional and radiological outcomes. Clin Orthop Surg 2022;14:367-74. [Google Scholar] [PubMed]
- 16. Mylle J, Burssens A, Fabry G. Simple bone cyst. A review of 59 cases with special reference to treatment. Acta Orthop Belg 1992;58:319-27. [Google Scholar] [PubMed]
- 17. Giannoudis PV, Dinopoulos H, Tsiridis E. Bone substitutes: An update. Injury 2005;36 Suppl 3:S20-7. [Google Scholar] [PubMed]
- 18. Agarwal A, Kumar D, Pal CP, Singh P, Sharma P. Surgical management of humeral unicameral bone cysts with internal fixation and bone grafting. J Clin Orthop Trauma 2023;38:102188. [Google Scholar] [PubMed]
- 19. Roposch A, Saraph V, Linhart WE. Treatment of unicameral bone cysts with demineralized bone matrix. J Bone Joint Surg Am 2000;82:1587-95. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report
July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis July 1, 2026 Novel Application of the AGN1 Triphasic Calcium-Based Implant for a Large Simple Bone Cyst in a Child With 3-Year Follow-up: A Case Report
July 1, 2026 Novel Application of the AGN1 Triphasic Calcium-Based Implant for a Large Simple Bone Cyst in a Child With 3-Year Follow-up: A Case Report July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report
July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report