
Humeral avulsion of the glenohumeral ligament (HAGL) lesion and associated soft tissue pathology shall be a part of the differential diagnosis in individuals presenting with persistent or unexplained shoulder instability for a better functional outcome.
Dr Prashu Ethirajan, Department of Arthroscopy and Sports Medicine, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600 116, Tamil Nadu, India. E-mail: prashuethirajan98@gmail.com
Abstract
Introduction: Humeral avulsion of the glenohumeral ligament (HAGL) is a rare but important cause of shoulder instability, often underdiagnosed due to subtle imaging findings and associated common injuries like rotator cuff tears, resulting in persistent pain, recurrent instability, and failure of conventional stabilisation procedures.
Case Report: We present a case of a 48-year-old male who sustained an anterior HAGL lesion with an associated subscapularis tear following a traumatic anterior shoulder displacement. Magnetic resonance imaging and arthroscopic visualisation confirmed the diagnosis. The patient underwent arthroscopic restoration of the anterior humeral avulsion of the glenohumeral ligament with knotless PEEK anchors. Postoperatively, the patient demonstrated better outcome scores and range of motion at 6-month follow-up.
Conclusion: Early identification and surgical repair of HAGL lesions are crucial in restoring shoulder stability, especially in active individuals. Arthroscopic techniques provide excellent visualisation and outcomes comparable to or superior to open repair when appropriately indicated.
Keywords: Humeral avulsion of the glenohumeral ligament, shoulder instability, arthroscopic repair, open repair, inferior glenohumeral ligament.
Humeral avulsion of the glenohumeral ligament (HAGL) was initially characterised by Wolf et al. in 1995 as a unique pathological entity associated with anterior shoulder instability and persistent pain, particularly in young and physically active individuals [1]. This injury results from avulsion of the inferior glenohumeral ligament (IGHL) complex since it’s humeral-accessory, thereby disrupting one of the primary static stabilisers of the glenohumeral joint. The stated predominance of HAGL lesions in the setting of traumatic anterior shoulder dislocations ranges from approximately 7–9%, although the true incidence is presumed to be higher due to underdiagnosis [2]. Clinically, patients commonly present with shoulder pain, instability, weakness, or recurrent episodes of dislocation, especially during movements involving abduction and external rotation. An elevated degree of clinical thought is essential for accurate diagnosis. Magnetic resonance imaging (MRI), particularly magnetic resonance arthrography (MRA), plays a key role in detecting HAGL lesions; however, these injuries are frequently underdiagnosed because concomitant pathologies, including rotator cuff tears as well as labral lesions, can divert clinical attention or obscure the characteristic imaging findings, which typically demonstrate the characteristic “J-sign”, which is suggestive of a HAGL lesion. Nevertheless, arthroscopy continues to be regarded as the definitive diagnostic modality [3,4,5]. We report the situation of a middle-aged male with an advanced HAGL lesion following a road traffic accident. HAGL lesions are frequently overlooked during the initial evaluation of traumatic shoulder instability. Neglected lesions may result in persistent pain, recurrent instability, and failure of conventional stabilisation procedures. Therefore, early recognition and appropriate administration are important to avert long-term functional impairment.
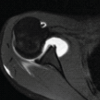
Our patient is a 48-year-old male driver who presented to the emergency department with pain and inability to move his right shoulder following a fall from a two-wheeler. He was found to have an anteriorly dislocated shoulder, which was confirmed with an X-ray and was reduced under sedation (Fig. 1). The patient had no similar episodes in the past. An MRI taken at a later date revealed an anterior HAGL lesion (J-sign positive) with an associated subscapularis tear and subluxated biceps tendon (Fig. 2).
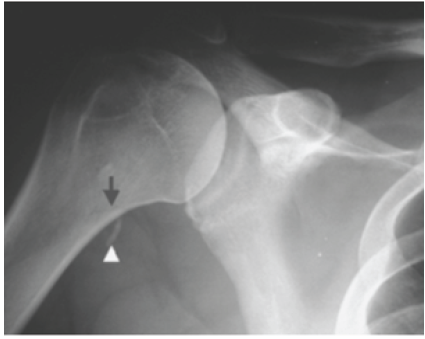
Figure 1: Plain radiograph demonstrating a bony humeral avulsion of the glenohumeral ligament lesion.
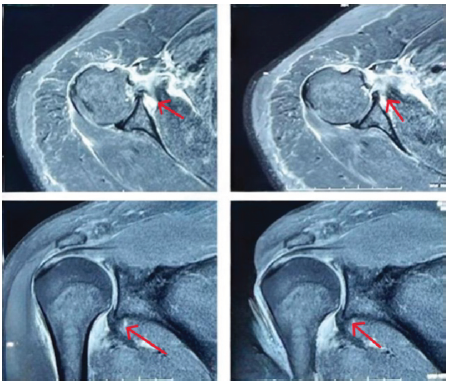
Figure 2: Magnetic resonance imaging demonstrating an anterior humeral avulsion of the glenohumeral ligament lesion with associated pathology.
Surgical technique:
We used a hydraulic traction device to put the patient’s right upper limb in traction and minor abduction under general anaesthesia and interscalene nerve block. The individual was positioned in the left lateral decubitus posture. We conducted diagnostic arthroscopy after establishing standard posterior, anterosuperior, and anteroinferior portals. Arthroscopic examination confirmed an anterior HAGL lesion by showing that the IGHL had detached from its humeral connection (Fig. 3).
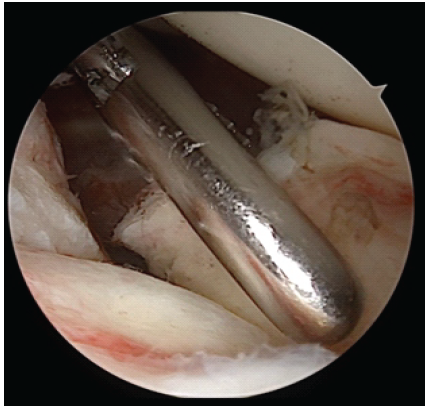
Figure 3: Diagnostic arthroscopy showing humeral avulsion of the glenohumeral ligament lesion.
The exposed humeral neck footprint was clearly visualised, along with associated pathology, including a subscapularis tear and medial subluxation of the extended head of the biceps tendon. The subluxated extended head of the biceps tendon was identified within the joint and temporarily secured away from the repair site after cinching with a no. 2 FiberWire suture (Fig. 4).

Figure 4: Medial subluxation of the long head of the biceps tendon.
Attention was then directed toward the IGHL repair. Sutures were passed through the avulsed IGHL using a suture passer, ensuring adequate tissue capture for anatomical restoration (Fig. 5).
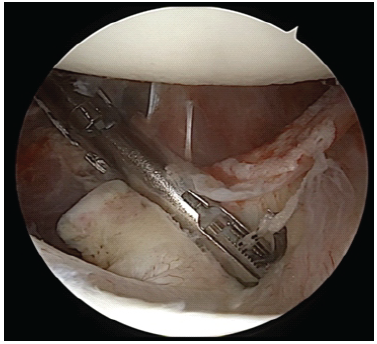
Figure 5: Suture passage through avulsed inferior glenohumeral ligament.
A 5 o’clock portal was recognised as laterally as possible and roughly 1 cm inferior to the upper edge of the subscapularis ligament, with the arm maintained in neutral rotation to reduce the risk of musculocutaneous nerve wound. The humeral head footprint of the IGHL was organised by a shaver to generate a bleeding bony surface to enable curing (Fig. 6).
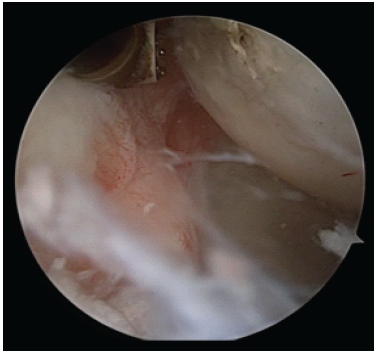
Figure 6: Preparation of humeral head footprint.
The IGHL was subsequently fixed to its anatomical footprint on the humeral skull using a 5.5 mm knotless PEEK anchor introduced through the 5 o’clock portal, with the anterosuperior portal serving as the viewing porch (Fig. 7).
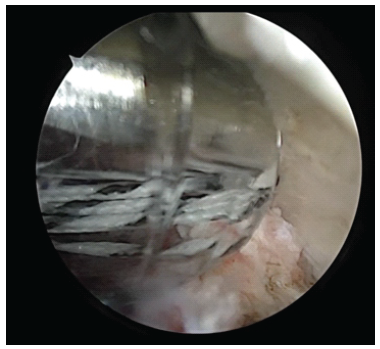
Figure 7: Inferior glenohumeral ligament fixation using a knotless anchor.
Upon probing, the repair was found to be stable, and restoration of the anterior capsuloligamentous tension was confirmed. The humeral head footprint of the subscapularis tendon was prepared. Subscapularis repair was done using No. 2 fibre wires and two 5.5 mm knotless PEEK anchors (Fig. 8).
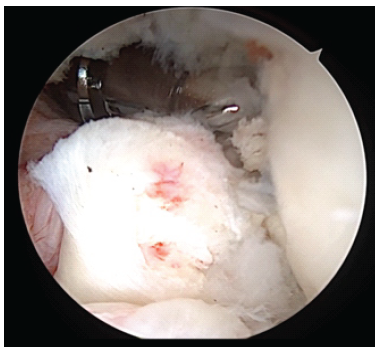
Figure 8: Subscapularis repair using a knotless PEEK anchor.
Subscapularis repair was found to be satisfactory. Notably, no labral tear was identified during arthroscopic evaluation, suggesting that the shoulder instability in this case was primarily related to the HAGL lesion in combination with the subscapularis tear rather than a Bankart-type lesion. Postoperatively, the individual was immobilised in a broad arm sling for 4 weeks to protect the repair. Passive range of motion was gradually initiated thereafter, beginning with Codman pendular exercises followed by active-assisted movements. Isometric strengthening exercises were commenced at 2 weeks post-surgery and progressively advanced to resistance band and isotonic strengthening as tolerated. By the end of 2 months, the patient had regained a near-full range of motion. Structured gym-based strengthening exercises were introduced at 3 months, and sport-specific and functional training was incorporated at 5 months postoperatively. At 6-month follow-up, the patient demonstrated marked functional improvement with significant gains in both patient-reported outcome measures and objective range of motion (Table 1).
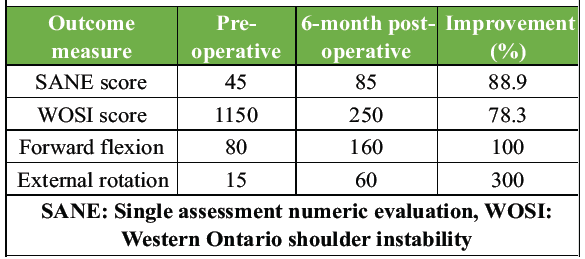
Table 1: Functional outcome analysis
The single assessment numeric evaluation (SANE) score improved from 45 preoperatively to 85 postoperatively, representing an 88.9% increase in perceived shoulder function. The Western Ontario shoulder instability (WOSI) score showed a 78.3% improvement, indicating a substantial reduction in pain, instability, and activity limitations. Forward flexion enhanced from 80° to 160°, effectively doubling the preoperative value, while external rotation showed the most pronounced improvement, increasing from 15° to 70°. These outcomes collectively reflect successful restoration of shoulder stability, mobility, and overall functional capacity following arthroscopic repair and structured rehabilitation. Notably, the patient, a professional driver, successfully returned to his occupational duties at 5 months postoperatively, representing an important return-to-work milestone. Formal quantitative shoulder strength testing using a dynamometer was not performed in this case, which is acknowledged as a limitation.
HAGL lesions represent an unusual but clinically important cause of persistent anterior shoulder instability, most commonly occurring after a traumatic anterior shoulder displacement. In the present case, a 48-year-old male sustained an anterior HAGL lesion with a concomitant subscapularis tear and a subluxated biceps tendon, which was managed through arthroscopic repair using knotless PEEK anchors. The patient achieved near-complete restoration of range of motion as well as function within 6 months, with marked improvements in SANE and WOSI scores. Compared with the existing literature, these outcomes align closely with previously reported favourable functional recoveries following both arthroscopic and open HAGL repairs [6]. In comparison, open repair has shown comparable results but with slightly higher recurrence rates over long-term follow-up. Dannaway et al. stated on 47 individuals undergoing open HAGL restoration, with a mean follow-up of 105 months, and noted a 21% recurrence of instability despite generally good WOSI scores and restored stability [7]. This suggests that while both techniques yield functional improvements, arthroscopic approaches may offer lower recurrence rates, possibly due to improved visualisation and minimally invasive access. It is also important to acknowledge that MRA is considered the preferred choice for HAGL lesion detection, offering superior sensitivity and specificity compared to conventional MRI, particularly for partial avulsions and subtle capsular injuries. In the present case, conventional MRI demonstrating the classic J-sign, coupled with definitive arthroscopic confirmation, provided a reliable diagnostic pathway; however, MRA would have offered enhanced preoperative delineation of lesion extent and associated pathology. Surgeons should consider MRA as the preferred pre-operative imaging tool in cases where conventional MRI findings are ambiguous. Moreover, the integration of associated pathology repair, as in the current case with subscapularis repair, is supported in the literature as a determinant of improved outcomes. Uppstorm et al. described collective arthroscopic rotator cuff repair and open HAGL restoration in older patients with multi-tendon involvement, demonstrating the value of addressing concurrent soft tissue injuries to restore full stability and motion [8]. Likewise, Liles et al. highlighted the “naked humeral head” scenario, where concurrent HAGL, subscapularis, and supraspinatus repairs produced excellent post-operative stability and function when all lesions were anatomically restored [9]. Biomechanically, repair of the IGHL has been shown to restore shoulder stability effectively. In cadaveric analysis, Park et al. demonstrated that large HAGL lesions led to significant increases in range of motion and translation, both of which were normalised after repair, confirming the stabilising role of the IGHL [10]. The present case, which showed restoration of the hammock effect post-repair, supports this biomechanical principle. In addition, Nicholson et al. reported return-to-sport rates of 93.5% after anterior HAGL repair, with 80% achieving pre-injury performance levels and low reoperation rates (6.2%) [11]. These findings, along with those from Nelson et al., who found 97% return to activity and significant pain reduction following surgery [12], suggest that operative management consistently produces durable, high-functioning outcomes across demographics. Overall, the present case mirrors the literature consensus that surgical repair of HAGL lesions – particularly when associated pathologies are addressed – yields excellent functional recovery, low recurrence, and substantial improvements in patient-reported outcomes. Arthroscopic repair with knotless anchors, as demonstrated here, provides an anatomic, minimally invasive, and biomechanically sound method for restoring stability and motion, even in older patients. Arthroscopic HAGL repair is a demanding procedure that requires advanced arthroscopic proficiency. The establishment of the accessory 5 o’clock anteroinferior portal carries a risk of injury to the musculocutaneous nerve, which was mitigated in this case by maintaining the arm in neutral rotation and placing the portal as laterally and superiorly as anatomically safe. Precise anchor placement at the humeral neck and suture passing in the inferior capsule are recognised risks that necessitate meticulous technique and appropriate implant selection. Post-operative shoulder stiffness is another potential complication, and the same was addressed through a structured, graduated rehabilitation programme. Surgeons inexperienced with inferior capsular work should be aware of these technical demands before attempting arthroscopic HAGL repair, and the procedure is recommended to be performed at centres with appropriate arthroscopic expertise.
Limitations:
The important limitations of this study have been highlighted in this section. This study represents a single-patient case report, and therefore, the findings cannot be generalised to the broader population of patients with HAGL lesions. The follow-up duration of 6 months, though sufficient to document early functional recovery, does not allow assessment of long-term shoulder stability, recurrence of instability, post-operative stiffness, or degenerative glenohumeral changes, and hence, longer follow-up is required. As there was no control group or comparison with open repair, the present report cannot establish the superiority of arthroscopic repair over other surgical techniques, and readers are requested to check the published comparative studies for evidence on relative technique efficacy [5,7]. Functional outcome assessment was limited to SANE and WOSI scores only, and additional validated outcome measures, such as the Constant–Murley score and ASES score, may be incorporated in future cases. Post-operative MRI or MRA was not performed to objectively confirm IGHL healing and anchor integration, given the excellent clinical recovery, but would be valuable for objective structural confirmation. The coexistence of subscapularis tear and biceps tendon subluxation makes it difficult to isolate the contribution of HAGL repair alone to the overall functional outcome; however, simultaneous repair of all identified pathology is consistent with established surgical principles and the available literature [8,9]. Post-operative quantitative shoulder strength testing was not performed; however, the patient returned to full occupational activities at 5 months. Pre-operative instability severity was assessed clinically but not quantified using objective laxity measurement tools, which limits pre-to-postoperative biomechanical comparison. The arthroscopic intraoperative size and extent of the HAGL lesion were not formally measured or classified, which may be relevant to surgical planning and prognosis in future cases. As with most published case series reporting successful surgical outcomes, selection bias toward favourable results cannot be excluded, and similarly, the findings of this case may not be directly applicable to elderly patients with poor tissue quality, chronic instability, or significant glenohumeral arthritis.
HAGL lesions, though uncommon, represent a critical source of shoulder instability. Early diagnosis using MRI or arthroscopy and appropriate surgical repair are essential for optimal outcomes. Objective and patient-reported gains indicate restoration of both pain-free mobility and perceived berm function succeeding arthroscopic reattachment of the IGHL and concurrent management of associated pathology. However, longer follow-up, objective strength assessment, postoperative imaging, and comparative studies are required to determine long-term stability and reproducibility of this technique.
Early surgical repair of the inferior glenohumeral tendon compound, along with the cure of concomitant lesions such as subscapularis tears, leads to reliable restoration of stability and shoulder function.
References
- 1. Wolf EM, Cheng JC, Dickson K. Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-7. [Google Scholar] [PubMed]
- 2. Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: The HAGL lesion. Am J Sports Med 2007;35:1960-6. [Google Scholar] [PubMed]
- 3. Varady NH, Retzky J, Reddy RP, Greditzer HG 4th, Tagliero AJ, Dines JS. Surgical management of humeral avulsion of the glenohumeral ligament injuries: Indications, treatment strategies, and outcomes. Curr Rev Musculoskelet Med 2025;18:281-8. [Google Scholar] [PubMed]
- 4. Grundshtein A, Kazum E, Chechik O, Dolkart O, Rath E, Bivas A, et al. Arthroscopic repair of humeral avulsion of glenohumeral ligament lesions: Outcomes at 2-year follow-up. Orthop J Sports Med 2021;9:23259671211004968. [Google Scholar] [PubMed]
- 5. Lee S, Krych AJ, Peebles AM, Rider D, Dekker TJ, Arner JW, et al. Outcomes of open versus arthroscopic treatment of HAGL tears. Am J Sports Med 2023;51:1581-7. [Google Scholar] [PubMed]
- 6. Markus DH, Morgan AM, Campbell KA, Alaia MJ, Jazrawi LM, Strauss EJ. Outcomes following arthroscopic repair of humeral avulsion of the glenohumeral ligament (HAGL) lesion: A systematic review. J Clin Orthop Traum 2023;41:102166. [Google Scholar] [PubMed]
- 7. Dannaway j, Raninga S, Bokor D. Long-term outcomes after open repair of humeral avulsion of the glenohumeral ligament. Orthop J Sports Med 2024;12:23259671241247544. [Google Scholar] [PubMed]
- 8. Uppstorm TJ, Jaber A, Dickinson NJ, Wang Y, Froom RJ, Cortes N, et al. Combined arthroscopic rotator cuff repair and open repair of humeral avulsion of glenohumeral ligament lesion: A surgical technique. Arthrosc Tech 2025;14:103793. [Google Scholar] [PubMed]
- 9. Liles JL, Fossum BW, Mologne M, Su CA, Godin JA. Treatment of the ‘The Naked Humeral Head’: Repair of supraspinatus avulsion, subscapularis tear, and humeral avulsion of the glenohumeral ligament. Arthrosc Tech 2022;11:e2103-11. [Google Scholar] [PubMed]
- 10. Park KJ, Tamboli M, Nguyen LY, McGarry MH, Lee TQ. A large humeral avulsion of the glenohumeral ligaments decreases stability that can be restored with repair. Clin Orthop Relat Res 2014;472:2372-9. [Google Scholar] [PubMed]
- 11. Nicholson TC, Sandler AB, Georger LA, Klahs KJ, Scanaliato JP, Hettrich CM, et al. Patients return to sport after repair of anterior humeral avulsion of the glenohumeral ligament lesions: A systematic review. JSES Rev Rep Tech 2024;4:359-64. [Google Scholar] [PubMed]
- 12. Nelson C, Reiter C, Cyrus J, Satalich J, O’Connell R, Vap A. Indications, management, and outcomes of humeral avulsions of the glenohumeral ligament: A systematic review. Orthop Rev (Pavia) 2022;14:37830. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Rare Presentation of Chronic Anterior Instability with Concomitant Triad of Anterior Labral Periosteal Sleeve Avulsion, Hill–Sachs, and Humeral Avulsion of the Glenohumeral Ligament Lesions: A Case Report
April 1, 2026 Rare Presentation of Chronic Anterior Instability with Concomitant Triad of Anterior Labral Periosteal Sleeve Avulsion, Hill–Sachs, and Humeral Avulsion of the Glenohumeral Ligament Lesions: A Case Report July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study
July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study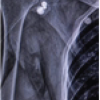 July 1, 2026 Single-Screw versus Two-Screw Fixation in the Latarjet Procedure: A Prospective Comparative Study
July 1, 2026 Single-Screw versus Two-Screw Fixation in the Latarjet Procedure: A Prospective Comparative Study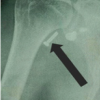 April 1, 2026 Eden-Hybinette Procedure as Salvage Treatment for Failed Latarjet Surgery: A Case Report
April 1, 2026 Eden-Hybinette Procedure as Salvage Treatment for Failed Latarjet Surgery: A Case Report